Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Sound Wall Starter KitDocument66 pagesSound Wall Starter KitMaxtron MoonPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 2 VCA ETT 2017 Training v2 0 - EnglishDocument129 pages2 VCA ETT 2017 Training v2 0 - EnglishMassimo FumarolaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Calculating Flow Through An Orifice Using ASME MFC-3M-1989 and Irrecoverable Pressure Drop EquationsDocument5 pagesCalculating Flow Through An Orifice Using ASME MFC-3M-1989 and Irrecoverable Pressure Drop EquationsRaphael212219Pas encore d'évaluation
- International Journal of Fatigue: SciencedirectDocument12 pagesInternational Journal of Fatigue: SciencedirectKurra SrikanthPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Form 1 Chapter 1 Introduction To ScienceDocument74 pagesForm 1 Chapter 1 Introduction To ScienceGooi Kee Win91% (43)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Positioning Ceramic Foam Filters in Gating System For Casting Alloy FiltrationDocument8 pagesPositioning Ceramic Foam Filters in Gating System For Casting Alloy FiltrationSiddharth GuptaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- رابع امتحانDocument81 pagesرابع امتحانraedabubaderPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
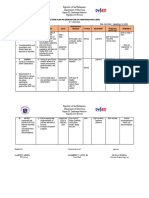
- Action Plan ESP 2023 24Document2 pagesAction Plan ESP 2023 24Je-Ann EstriborPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Lecture Week 5 - Confidence Intervals Hypothesis Testing and PvaluesDocument49 pagesLecture Week 5 - Confidence Intervals Hypothesis Testing and PvalueshgfmefPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
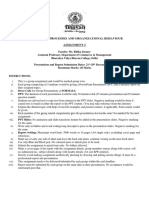
- MPOB Assignment 2 - Group PresentationsDocument4 pagesMPOB Assignment 2 - Group PresentationsSonalika BhambiPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Yan Li 2016Document10 pagesYan Li 2016Hendy Dwi WarmikoPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- 106 20170705 Method Statement For ExcavationDocument17 pages106 20170705 Method Statement For ExcavationEmad RakatPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Subject: Political Science I Course: Ba LLB Semester I Lecturer: Ms. Deepika Gahatraj Module: Module Iv, Theories of The Origin of StateDocument4 pagesSubject: Political Science I Course: Ba LLB Semester I Lecturer: Ms. Deepika Gahatraj Module: Module Iv, Theories of The Origin of StateSuzette OratPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Ameh FRSC FormDocument3 pagesAmeh FRSC FormULOKO CHRISTIANPas encore d'évaluation
- Nonlinear Vibration Isolation Via A Compliant Mechanism and Wire RopesDocument16 pagesNonlinear Vibration Isolation Via A Compliant Mechanism and Wire Ropesali salekifardPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Research Paper 3 PDFDocument28 pagesResearch Paper 3 PDFSushmaSahuPas encore d'évaluation
- EF3e Intplus Filetest 4aDocument7 pagesEF3e Intplus Filetest 4aЯна ИвановаPas encore d'évaluation
- 4.4.1.4 DLL - ENGLISH-6 - Q4 - W4.docx Version 1Document13 pages4.4.1.4 DLL - ENGLISH-6 - Q4 - W4.docx Version 1Gie Escoto Ocampo100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Human Development: A Re-Education in Freedom, Love and Happiness by Patrick WhelanDocument174 pagesHuman Development: A Re-Education in Freedom, Love and Happiness by Patrick WhelanPatrick WhelanPas encore d'évaluation
- Chemical WarfareDocument18 pagesChemical WarfareUnited States Militia100% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Stratos DR. DMS D.esintrometroDocument14 pagesStratos DR. DMS D.esintrometroRosa Aldiris Garcia MedranoPas encore d'évaluation
- A Blessing and A Curse CEO Empathy by Andreas Konig - Case DownloadedDocument25 pagesA Blessing and A Curse CEO Empathy by Andreas Konig - Case Downloadedsarthak sethPas encore d'évaluation
- Issue: 3D at Depth: The Future Is GreenDocument72 pagesIssue: 3D at Depth: The Future Is GreenPepePas encore d'évaluation
- On NCVET FunctioningDocument35 pagesOn NCVET Functioningsingh.darshan9100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- OverthinkingDocument9 pagesOverthinkinghabibatullah nur hanifahPas encore d'évaluation
- Contoh Sterilefiltration Pada Viral Vaccine Live AtenuatedDocument10 pagesContoh Sterilefiltration Pada Viral Vaccine Live Atenuatedkomang inggasPas encore d'évaluation
- QM For Business MIDTERM EXAMINATION REVIEW Apr 23 2020 BULLSHIT CONTENTDocument10 pagesQM For Business MIDTERM EXAMINATION REVIEW Apr 23 2020 BULLSHIT CONTENTArgen GrzesiekPas encore d'évaluation
- Director For GADDocument4 pagesDirector For GADSultan Kudarat State UniversityPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- BUS 8375 Lec. 11 Assignment 4 Qualitative Analysis v.1 1Document8 pagesBUS 8375 Lec. 11 Assignment 4 Qualitative Analysis v.1 1Jaspal SinghPas encore d'évaluation
- Choice TheoryDocument2 pagesChoice Theoryginabonieve100% (1)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)