Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Health Communication and Mass Media CH1 PDFDocument17 pagesHealth Communication and Mass Media CH1 PDFShamsa KanwalPas encore d'évaluation
- Acute Renal FailureDocument15 pagesAcute Renal FailureJoe RealPas encore d'évaluation
- 5 Vol3 Issue3 MS 15175Document8 pages5 Vol3 Issue3 MS 15175kanna_dhasan25581Pas encore d'évaluation
- 13-5-2010 MCQ FrcaDocument79 pages13-5-2010 MCQ FrcaMohmd Abdulhameed Sayed100% (2)
- Revised Instrument Packet 2Document44 pagesRevised Instrument Packet 2Abdiaziz Walhad0% (1)
- Dispensing MedicinesDocument80 pagesDispensing Medicinesfa6oom1994Pas encore d'évaluation
- Pearls in PPCDocument5 pagesPearls in PPCRajinder Kumar BassanPas encore d'évaluation
- Healing ArchitectureDocument5 pagesHealing ArchitectureSUDHAKARMANI100% (2)
- New Hope For A Cure To Liver CirrhosisDocument2 pagesNew Hope For A Cure To Liver Cirrhosissina_bopol100% (1)
- Diaphragm: Surgical Anatomy of The DiaphragmDocument14 pagesDiaphragm: Surgical Anatomy of The DiaphragmOlga CerlatPas encore d'évaluation
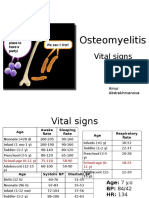
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaPas encore d'évaluation
- Understanding Behavior-A Key To DisciplineDocument1 pageUnderstanding Behavior-A Key To Disciplinemakcin_cyril314250% (2)
- Changing Epidemiology of Upper Gastrointestinal Hemorrhage in The Last DecadeDocument8 pagesChanging Epidemiology of Upper Gastrointestinal Hemorrhage in The Last DecadeAlline CastroPas encore d'évaluation
- Ulnar Nerve Injury, Diagnosis and TreatmentDocument30 pagesUlnar Nerve Injury, Diagnosis and TreatmentsherysheryyPas encore d'évaluation
- Cute Baby: Ashroff Memorial Hospital Ward 03Document27 pagesCute Baby: Ashroff Memorial Hospital Ward 03dhanushkaPas encore d'évaluation
- Stroke: Lynn Wittwer, MD, MPD Clark County EMSDocument35 pagesStroke: Lynn Wittwer, MD, MPD Clark County EMSvorez100% (1)
- Selective Grinding in Complete DentureDocument10 pagesSelective Grinding in Complete Denturevarun100% (1)
- Anxiety Dissorder PDFDocument273 pagesAnxiety Dissorder PDFdnaPas encore d'évaluation
- "Psychology Works" Fact Sheet:: Obsessive Compulsive DisorderDocument4 pages"Psychology Works" Fact Sheet:: Obsessive Compulsive DisorderDedy HariwijayaPas encore d'évaluation
- Nursing Diagnosis of Prostate CancerDocument3 pagesNursing Diagnosis of Prostate CancerSyafiqAzizi100% (1)
- 柳奇學姐提供的Mode of Mechanical VentilatorDocument79 pages柳奇學姐提供的Mode of Mechanical Ventilatorapi-25944730100% (10)
- Potts Disease NCP .. JustificationDocument8 pagesPotts Disease NCP .. JustificationMicah SalesPas encore d'évaluation
- Benchmark Ethical Decision MakingDocument5 pagesBenchmark Ethical Decision Makingapi-509678368Pas encore d'évaluation
- FS13 PolycythemiaVera FactSheetDocument7 pagesFS13 PolycythemiaVera FactSheetMala 'emyu' UmarPas encore d'évaluation
- Strickland PresentationDocument1 pageStrickland Presentationmariopi2495Pas encore d'évaluation
- Vertigo DavidsonDocument13 pagesVertigo DavidsonifahInayahPas encore d'évaluation
- Chronic UrticariaDocument40 pagesChronic UrticariaeeeeewwwwwPas encore d'évaluation
- Care Map UtiDocument1 pageCare Map UtiJonathonPas encore d'évaluation
- Medical Vocabulary - HOSPITALDocument4 pagesMedical Vocabulary - HOSPITALBianca AndreeaPas encore d'évaluation
- What Are Moral DilemmasDocument7 pagesWhat Are Moral DilemmasMary Anne Rocafor NaelgasPas encore d'évaluation