Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Resistance Loop Band - Workout GuideDocument41 pagesResistance Loop Band - Workout GuideSanjay GharatPas encore d'évaluation
- Warrior ZeroDocument46 pagesWarrior ZeroKevin100% (2)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Forever Fix Exercise Manual Phase 2 PDFDocument35 pagesThe Forever Fix Exercise Manual Phase 2 PDFmarellja100% (1)
- Functional: Body CompositionDocument49 pagesFunctional: Body CompositionMnawer Hadid100% (11)
- Barbell Workouts Vol 2 2020Document23 pagesBarbell Workouts Vol 2 2020Alberone jr100% (1)
- CoachWoot Body Beast Workout Tracking Sheet Schedule WorksheetDocument12 pagesCoachWoot Body Beast Workout Tracking Sheet Schedule WorksheetThinh- XukaPas encore d'évaluation
- Foundations of Periodization and Program Design Course Notes PDFDocument109 pagesFoundations of Periodization and Program Design Course Notes PDFv89% (9)
- Legs Specialization PDFDocument7 pagesLegs Specialization PDFmylo299Pas encore d'évaluation
- Mad Skills WorkbookDocument18 pagesMad Skills WorkbookMurad Almjresi100% (5)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- 6 Week Powerlifting ProgramDocument7 pages6 Week Powerlifting ProgramKitaan ReddyPas encore d'évaluation
- Weightlifting USAW Level 1 Sports PerformanceDocument50 pagesWeightlifting USAW Level 1 Sports PerformanceChris Kasinski100% (2)
- Kettlebell Secrets Special ReportDocument10 pagesKettlebell Secrets Special Reportpopeyeballina78% (9)
- Reform - The 12-Week Transformation Workout Plan - Muscle & FitnessDocument17 pagesReform - The 12-Week Transformation Workout Plan - Muscle & FitnessDeejay ShivPas encore d'évaluation
- Basic Weight Lifting Exercises PDFDocument6 pagesBasic Weight Lifting Exercises PDFGerald KwinjoPas encore d'évaluation
- Optimal Nutrition For ExerciseDocument19 pagesOptimal Nutrition For ExerciseEashwar Prasad Meenakshi100% (2)
- 34 Pictures To See Which Muscle You Are StretchingDocument16 pages34 Pictures To See Which Muscle You Are Stretchinggprasadatvu100% (1)
- (Laura Lee (Dolly) Swisher PT PHD, Catherine G. P PDFDocument228 pages(Laura Lee (Dolly) Swisher PT PHD, Catherine G. P PDFmemonsabaa61100% (1)
- The Bear and Two FriendsDocument1 pageThe Bear and Two FriendsEashwar Prasad MeenakshiPas encore d'évaluation
- RH Fever PDFDocument5 pagesRH Fever PDFEashwar Prasad MeenakshiPas encore d'évaluation
- Pneumonia by MepDocument5 pagesPneumonia by MepEashwar Prasad MeenakshiPas encore d'évaluation
- Stroke PDFDocument3 pagesStroke PDFEashwar Prasad MeenakshiPas encore d'évaluation
- Tennis ElbowDocument5 pagesTennis ElbowEashwar Prasad MeenakshiPas encore d'évaluation
- PH Iotherap Hi Tor : Early History of PhysiotherapyDocument5 pagesPH Iotherap Hi Tor : Early History of PhysiotherapyEashwar Prasad MeenakshiPas encore d'évaluation
- Cervical Traction 2Document13 pagesCervical Traction 2Dw Ipha Ma HaPas encore d'évaluation
- Systemic SclerosisDocument3 pagesSystemic SclerosisEashwar Prasad MeenakshiPas encore d'évaluation
- Stroke PDFDocument3 pagesStroke PDFEashwar Prasad MeenakshiPas encore d'évaluation
- PSORIASISDocument3 pagesPSORIASISEashwar Prasad MeenakshiPas encore d'évaluation
- Systemic SclerosisDocument3 pagesSystemic SclerosisEashwar Prasad MeenakshiPas encore d'évaluation
- Spondylolisthesis PDFDocument3 pagesSpondylolisthesis PDFEashwar Prasad MeenakshiPas encore d'évaluation
- Spina BifidaDocument4 pagesSpina BifidaEashwar Prasad MeenakshiPas encore d'évaluation
- SP - Cord Inj - Para) QuaDocument7 pagesSP - Cord Inj - Para) QuaEashwar Prasad MeenakshiPas encore d'évaluation
- Pneumonia by MepDocument5 pagesPneumonia by MepEashwar Prasad MeenakshiPas encore d'évaluation
- Sciatica Ortho PivdDocument3 pagesSciatica Ortho PivdEashwar Prasad MeenakshiPas encore d'évaluation
- PDADocument3 pagesPDAEashwar Prasad MeenakshiPas encore d'évaluation
- Plantarfascitiscal &Document4 pagesPlantarfascitiscal &Eashwar Prasad MeenakshiPas encore d'évaluation
- PT Ortho VsqsaDocument4 pagesPT Ortho VsqsaEashwar Prasad MeenakshiPas encore d'évaluation
- PoliomyelitisDocument3 pagesPoliomyelitisEashwar Prasad MeenakshiPas encore d'évaluation
- PTManagement Lumbar PDFDocument2 pagesPTManagement Lumbar PDFEashwar Prasad MeenakshiPas encore d'évaluation
- P D BymepgoogledriveDocument10 pagesP D BymepgoogledriveEashwar Prasad MeenakshiPas encore d'évaluation
- Pa PDFDocument2 pagesPa PDFEashwar Prasad MeenakshiPas encore d'évaluation
- P DSDocument5 pagesP DSEashwar Prasad MeenakshiPas encore d'évaluation
- Osteomyelitis MepdrDocument4 pagesOsteomyelitis MepdrEashwar Prasad MeenakshiPas encore d'évaluation
- Ortho Vsaqs by MpmepDocument28 pagesOrtho Vsaqs by MpmepEashwar Prasad MeenakshiPas encore d'évaluation
- Oct 15 Vsaqs BiomechDocument4 pagesOct 15 Vsaqs BiomechEashwar Prasad MeenakshiPas encore d'évaluation
- NEURODocument6 pagesNEUROEashwar Prasad MeenakshiPas encore d'évaluation
- The Tight Tan Slacks of Dezso Ban - Learning To Prevent Injuries - Richard WinettDocument4 pagesThe Tight Tan Slacks of Dezso Ban - Learning To Prevent Injuries - Richard WinettCD KHUTIYALEPas encore d'évaluation
- Adidas Manchester Marathon 2023 Training Plan AdvancedDocument13 pagesAdidas Manchester Marathon 2023 Training Plan AdvancedMohamed ChedlyPas encore d'évaluation
- Circuit TrainingDocument2 pagesCircuit Trainingshelbs32Pas encore d'évaluation
- ELK FIT Program PDF WebDocument12 pagesELK FIT Program PDF WebDavid EhrhardtPas encore d'évaluation
- Madbarz Routines Plan Expert-Cardio&StrengthDocument20 pagesMadbarz Routines Plan Expert-Cardio&StrengthJuan Sebastian AnguloPas encore d'évaluation
- The WeighTrainer - Beginners - Practical Starting Routines For The Drug-Free TraineeDocument12 pagesThe WeighTrainer - Beginners - Practical Starting Routines For The Drug-Free Traineebarna284Pas encore d'évaluation
- Air Alert 4Document6 pagesAir Alert 4GabrielePas encore d'évaluation
- MFT Cycle 5 OpenDocument45 pagesMFT Cycle 5 OpennickmasiusPas encore d'évaluation
- The Only 12 Exercises You Need To Get in ShapeDocument36 pagesThe Only 12 Exercises You Need To Get in Shapess87622Pas encore d'évaluation
- RESULTS FITNESS TRANSFORMATIONDocument20 pagesRESULTS FITNESS TRANSFORMATIONBlowkeePas encore d'évaluation
- Lesson Plan Air SquatDocument6 pagesLesson Plan Air Squatapi-443381963Pas encore d'évaluation
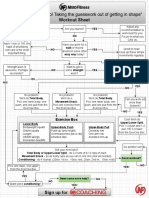
- Tell Me What To Do Flowchart V2 PDFDocument3 pagesTell Me What To Do Flowchart V2 PDFFernando Stuar Campos MendozaPas encore d'évaluation
- Matt Roberts 2 Week Blitz - Sheet1Document2 pagesMatt Roberts 2 Week Blitz - Sheet1Paddy MehargPas encore d'évaluation
- ThrowingDocument14 pagesThrowingmikotaktPas encore d'évaluation
- Second QuarterDocument5 pagesSecond QuarterCarlo Bryan RamentoPas encore d'évaluation