Vous aimerez peut-être aussi
- Pathology - Chapter 4Document9 pagesPathology - Chapter 4Cory GrayPas encore d'évaluation
- Diseases Involving Blood Vessels of The KidneysDocument34 pagesDiseases Involving Blood Vessels of The KidneysAma SatharasinghePas encore d'évaluation
- VasculitisDocument42 pagesVasculitissamaPas encore d'évaluation
- Tubulointerstitial Nephritis BharatDocument12 pagesTubulointerstitial Nephritis Bharatgauravsingh708284Pas encore d'évaluation
- Acute Tubular Necrosis 2Document19 pagesAcute Tubular Necrosis 2Sangeeta BSRPas encore d'évaluation
- ENDOCRINE HYPERTENSION. A Number of Hormonal Secretions May Produce Secondary HyDocument5 pagesENDOCRINE HYPERTENSION. A Number of Hormonal Secretions May Produce Secondary HyIsak ShatikaPas encore d'évaluation
- Week 1Document10 pagesWeek 1Supipi GamagePas encore d'évaluation
- RENAL VASCULAR DISEASES UpdatedDocument97 pagesRENAL VASCULAR DISEASES UpdatedgibreilPas encore d'évaluation
- Pathoma Lecture Notes 2017Document42 pagesPathoma Lecture Notes 2017Priyesh PrincePas encore d'évaluation
- Acute Tubular NecrosisDocument15 pagesAcute Tubular NecrosisDeepak patelPas encore d'évaluation
- 5.the Kidney - 5Document19 pages5.the Kidney - 5madhuPas encore d'évaluation
- Chapter (1) Blood VesselsDocument16 pagesChapter (1) Blood VesselsyuhazikrillahPas encore d'évaluation
- 9 - Nephrotic SyndromeDocument5 pages9 - Nephrotic SyndromeAbdallah Essam Al-ZireeniPas encore d'évaluation
- Jurnal Penyakit Jantung Koroner: Nama: Besse Saika Nirmalasari KLS: W8 STB: 1412090440Document15 pagesJurnal Penyakit Jantung Koroner: Nama: Besse Saika Nirmalasari KLS: W8 STB: 1412090440Wardiansyah NaimPas encore d'évaluation
- Etiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDateDocument22 pagesEtiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDatecuentaparatrabajosdelau10Pas encore d'évaluation
- Venous Thromboembolic DiseaseDocument27 pagesVenous Thromboembolic DiseaseAndra BauerPas encore d'évaluation
- Lab 15 Nerki 2020 - 21Document175 pagesLab 15 Nerki 2020 - 21Dominika WaligóraPas encore d'évaluation
- Ερωτήσεις διάφορεςDocument108 pagesΕρωτήσεις διάφορεςyiafkaPas encore d'évaluation
- Syahirah's Essay - InfarctDocument2 pagesSyahirah's Essay - InfarctNursyahirah IshakPas encore d'évaluation
- Acute Coronary Syndrome: Aminah DalimuntheDocument48 pagesAcute Coronary Syndrome: Aminah Dalimunthesintesis obatPas encore d'évaluation
- 3 Renal Vascular Disease 3Document46 pages3 Renal Vascular Disease 3Coy NuñezPas encore d'évaluation
- Pathology RCR1 CardioDocument6 pagesPathology RCR1 CardioeamcrawleyPas encore d'évaluation
- Lecture 5Document5 pagesLecture 5Isak ShatikaPas encore d'évaluation
- Cerebral VasculitisDocument46 pagesCerebral VasculitisMatteo PaolucciPas encore d'évaluation
- Kidney and Urinary Tract Pathology: Dr. Dr. Delyuzar, M.Ked (Pa), Sppa (K) Dr. Dr. Lidya Imelda Laksmi, M.Ked (Pa), SppaDocument40 pagesKidney and Urinary Tract Pathology: Dr. Dr. Delyuzar, M.Ked (Pa), Sppa (K) Dr. Dr. Lidya Imelda Laksmi, M.Ked (Pa), Sppaangelica gloryPas encore d'évaluation
- Disseminated Intravascular Coagulation (DIC)Document14 pagesDisseminated Intravascular Coagulation (DIC)Mohamed AlmahadiPas encore d'évaluation
- VasculitisDocument184 pagesVasculitisRada NemirovskiPas encore d'évaluation
- Diseases of The Blood VesselsDocument2 pagesDiseases of The Blood VesselsGlogogeanu Cristina AndreeaPas encore d'évaluation
- Curs Bolile PericarduluiDocument85 pagesCurs Bolile PericarduluiAndreea ElenaPas encore d'évaluation
- ABC Acute Renal FailureDocument5 pagesABC Acute Renal FailureAngela CristinoPas encore d'évaluation
- Lo Week 2-1Document8 pagesLo Week 2-1Martien Silviandy SetiawanPas encore d'évaluation
- Pathology+101 Complete)Document147 pagesPathology+101 Complete)Goh Kah Yong100% (2)
- Infective EndocarditisDocument10 pagesInfective EndocarditisShrests SinhaPas encore d'évaluation
- باثو 2Document35 pagesباثو 2shahadkhaled171Pas encore d'évaluation
- 3 FullDocument13 pages3 Fullمحمد رافد لطيفPas encore d'évaluation
- Lecture #5 - Circulatory DisturbanceDocument36 pagesLecture #5 - Circulatory DisturbanceEl Farouk100% (1)
- PathologyDocument48 pagesPathologyMaya KawwaPas encore d'évaluation
- Peripheral Vascular DiseaseDocument61 pagesPeripheral Vascular DiseaseAkash ShillPas encore d'évaluation
- Deep Vein ThrombosisDocument19 pagesDeep Vein ThrombosisDoctor MusicPas encore d'évaluation
- Reduced Renal Sodium Excretion: Forced Through A Narrow LumenDocument5 pagesReduced Renal Sodium Excretion: Forced Through A Narrow LumenFlowerPas encore d'évaluation
- Hypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TDocument44 pagesHypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TUsaid SulaimanPas encore d'évaluation
- Acute Kidney InjuryDocument20 pagesAcute Kidney InjuryTishya MukherjeePas encore d'évaluation
- Hemostatic Complications of Solid OrganDocument18 pagesHemostatic Complications of Solid OrganWael AlkhiaryPas encore d'évaluation
- Palliative Care in DMDocument35 pagesPalliative Care in DMSyifa Hasna NadiaPas encore d'évaluation
- Glomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimDocument53 pagesGlomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimnadddPas encore d'évaluation
- (Template) DVTDocument21 pages(Template) DVTPema Lamu TdkPas encore d'évaluation
- DB50 - Pa Tho Physiology and Pathology of ShockDocument4 pagesDB50 - Pa Tho Physiology and Pathology of ShockChelsea RosePas encore d'évaluation
- End Stage Renal DiseaseDocument6 pagesEnd Stage Renal DiseaseLeiPas encore d'évaluation
- Myocardial InfarctionDocument47 pagesMyocardial Infarctionsanjesh1100% (2)
- Hemodynamic Disorder PC1Document227 pagesHemodynamic Disorder PC1Bereket weybaPas encore d'évaluation
- Chronic Kidney DiseaseDocument20 pagesChronic Kidney DiseasePappu HSD VenkateshPas encore d'évaluation
- Hemodynamic Disorders, Thrombosis and ShockDocument127 pagesHemodynamic Disorders, Thrombosis and ShockMowlidAbdirahman Ali madaalePas encore d'évaluation
- Endothelin Renal Diseases and Hypertension PDFDocument7 pagesEndothelin Renal Diseases and Hypertension PDFElena EllaPas encore d'évaluation
- Tinjauan Pustaka: Winsa Husin, Otje Hudaja, Yusak KristiantoDocument44 pagesTinjauan Pustaka: Winsa Husin, Otje Hudaja, Yusak KristiantoAnonymous GsJNLmbwkXPas encore d'évaluation
- Cirrhosis: DR AkhondeiDocument111 pagesCirrhosis: DR AkhondeiMuvenn KannanPas encore d'évaluation
- Hemorrhage Lec 1Document30 pagesHemorrhage Lec 1balachris64Pas encore d'évaluation
- 4th Auguest 2016 Fluid and Hemodynamic Disorders 2011Document81 pages4th Auguest 2016 Fluid and Hemodynamic Disorders 2011Majkel Benche Custodio MllPas encore d'évaluation
- Disturbances in The Blood Flow1Document41 pagesDisturbances in The Blood Flow1ammar amerPas encore d'évaluation
- Practice Problems I.V (Autosaved) (Autosaved)Document56 pagesPractice Problems I.V (Autosaved) (Autosaved)Walaa abo foolPas encore d'évaluation
- Drug-Body Interactions IncludeDocument45 pagesDrug-Body Interactions IncludeWalaa abo foolPas encore d'évaluation
- Chapter 6 DiabetesDocument66 pagesChapter 6 DiabetesWalaa abo foolPas encore d'évaluation
- Bioavailability and BioequivalenceDocument53 pagesBioavailability and BioequivalenceWalaa abo foolPas encore d'évaluation
- Pharmaceutical GranulesDocument55 pagesPharmaceutical GranulesWalaa abo foolPas encore d'évaluation
- Lecture 18 SuppositoriesDocument2 pagesLecture 18 SuppositoriesWalaa abo foolPas encore d'évaluation
- TabletsDocument104 pagesTabletsWalaa abo foolPas encore d'évaluation
- محاضرة 28 PDFDocument15 pagesمحاضرة 28 PDFWalaa abo foolPas encore d'évaluation
- Soft Gelatin CapsulesDocument74 pagesSoft Gelatin CapsulesWalaa abo fool100% (1)
- Pharmaceutical GranulesDocument55 pagesPharmaceutical GranulesWalaa abo fool100% (1)
- Biol 309 Question Bank Cell CommunicationDocument6 pagesBiol 309 Question Bank Cell CommunicationWalaa abo fool100% (1)
- Glomerular Diseases: Membrano Proliferative Glomerulonephritis (MPGN) - in This LectureDocument12 pagesGlomerular Diseases: Membrano Proliferative Glomerulonephritis (MPGN) - in This LectureWalaa abo foolPas encore d'évaluation
- BB BS Enzyme49Document36 pagesBB BS Enzyme49Walaa abo foolPas encore d'évaluation
- Water and Buffer L-2Document42 pagesWater and Buffer L-2Walaa abo foolPas encore d'évaluation
- Medicine: CardiorespiratoryDocument56 pagesMedicine: CardiorespiratoryWalaa abo foolPas encore d'évaluation
- Voiding Dysfunction U06-U11.: 1. Urinary RetentionDocument7 pagesVoiding Dysfunction U06-U11.: 1. Urinary RetentionFarah FarahPas encore d'évaluation
- Malignant Small Round Cell TumorsDocument12 pagesMalignant Small Round Cell TumorsSaptarshi Ghosh100% (1)
- 18 Cellular AberrationsDocument70 pages18 Cellular AberrationsBea Bianca CruzPas encore d'évaluation
- A Case Report of Wilms TumorDocument3 pagesA Case Report of Wilms TumorAna LyanaPas encore d'évaluation
- 3 - Pediatric Wilms' TumorDocument5 pages3 - Pediatric Wilms' TumorDiana MitreaPas encore d'évaluation
- Class Teaching On Wilms TumourDocument32 pagesClass Teaching On Wilms TumourKayal GuruPas encore d'évaluation
- NCA1Document12 pagesNCA1Ley BeltranPas encore d'évaluation
- Cellular Aberrations (Basic Concepts of Oncology)Document12 pagesCellular Aberrations (Basic Concepts of Oncology)PATRIZJA YSABEL REYESPas encore d'évaluation
- Minimally Invasive Surgery in Pediatric Oncology Galazka 2019Document11 pagesMinimally Invasive Surgery in Pediatric Oncology Galazka 2019jonays_0106293Pas encore d'évaluation
- Scanning Technique of KidneysDocument103 pagesScanning Technique of KidneysPhuntsho OngmoPas encore d'évaluation
- SEMINAR On Pediatric OncologyDocument133 pagesSEMINAR On Pediatric Oncologysheenakuttu100% (1)
- Protocol SIOP 2001Document171 pagesProtocol SIOP 2001Omar Bendriss AlamiPas encore d'évaluation
- Wilms Tumor Imaging - Overview, Radiography, Computed TomographyDocument24 pagesWilms Tumor Imaging - Overview, Radiography, Computed TomographyVela NazarPas encore d'évaluation
- Askep Tumor Wilms: Ni Nyoman Udiani, S.Kep - Ns.,M.KepDocument36 pagesAskep Tumor Wilms: Ni Nyoman Udiani, S.Kep - Ns.,M.KepRelysa Magdalena IssiPas encore d'évaluation
- Pediatric CancerDocument73 pagesPediatric CancerAnna Mae DollentePas encore d'évaluation
- Wilms' Tumor: By: Feniel Alquizar Aldin PiamonteDocument23 pagesWilms' Tumor: By: Feniel Alquizar Aldin PiamonteNalzaro EmyrilPas encore d'évaluation
- Ped Anesth 16 (504-13) 2006Document10 pagesPed Anesth 16 (504-13) 2006linhohb4833Pas encore d'évaluation
- Pediatric Solid TumorsDocument43 pagesPediatric Solid Tumorsririliberti100% (1)
- Wilms Tumor NelsonDocument8 pagesWilms Tumor NelsonvegaPas encore d'évaluation
- Wilms Tumor OverviewDocument23 pagesWilms Tumor OverviewJenn100% (2)
- Tumors of Kidney: Dr.K.Sathish Kumar, MD (Hom) .Document10 pagesTumors of Kidney: Dr.K.Sathish Kumar, MD (Hom) .mnr hmcPas encore d'évaluation
- REVALIDADocument53 pagesREVALIDAMercy Anne EcatPas encore d'évaluation
- Wilm's Tumor Nclex Questions (Sulong)Document3 pagesWilm's Tumor Nclex Questions (Sulong)Christinajunior ASPas encore d'évaluation
- Advanced Clinical Problem Solving Transition Into Nursing PracticeDocument55 pagesAdvanced Clinical Problem Solving Transition Into Nursing PracticeZarida ArabainPas encore d'évaluation
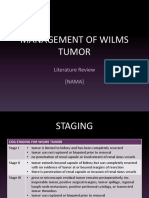
- Management of Wilms Tumor: Literature Review (NAMA)Document15 pagesManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaPas encore d'évaluation
- Wilms TumourDocument3 pagesWilms TumourfifahcantikPas encore d'évaluation
- SolidtumorsinchildrenDocument24 pagesSolidtumorsinchildrenPriyaPas encore d'évaluation
- Wilms TumorDocument12 pagesWilms TumorKath CamachoPas encore d'évaluation
- Wilms Tumour: Nitha K 2 Year MSC NursingDocument40 pagesWilms Tumour: Nitha K 2 Year MSC NursingNITHA K100% (1)
- Solid TumoursDocument48 pagesSolid TumoursViswanadh BPas encore d'évaluation