Vous aimerez peut-être aussi
- Fractional CO2Document11 pagesFractional CO2Dokter RudyPas encore d'évaluation
- The Puzzle of Urticaria - International Research AbstractsD'EverandThe Puzzle of Urticaria - International Research AbstractsPas encore d'évaluation
- In AdditionDocument3 pagesIn AdditionKramer ChangPas encore d'évaluation
- Nottingham City HospitalDocument5 pagesNottingham City HospitaljohnmarcPas encore d'évaluation
- Benign and Premalignant Skin Lesions.31Document11 pagesBenign and Premalignant Skin Lesions.31rafafpsPas encore d'évaluation
- Actinic Cheratosis - A ReviewDocument4 pagesActinic Cheratosis - A ReviewMARIUS-MIRCEA POPESCU-MICLOSANUPas encore d'évaluation
- Review in Peeling ComplicationsDocument8 pagesReview in Peeling ComplicationschipanzePas encore d'évaluation
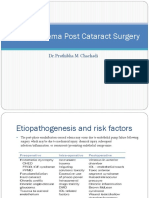
- Corneal Edema Post Cataract SurgeryDocument13 pagesCorneal Edema Post Cataract SurgeryPrathibha M ChachadiPas encore d'évaluation
- Recent Advances in OtorhinolaryngologyDocument22 pagesRecent Advances in OtorhinolaryngologyInderdeep Arora100% (1)
- Burns InjuryDocument23 pagesBurns Injurymary_chdhry100% (1)
- Ax00cwavtu34vwcn - Practical Management of Common Skin Injuries Lacerations Wounds Trigger Fingers and BurnsDocument10 pagesAx00cwavtu34vwcn - Practical Management of Common Skin Injuries Lacerations Wounds Trigger Fingers and BurnsEvelyn AtuyaPas encore d'évaluation
- Management Ulkus KorneaDocument8 pagesManagement Ulkus Korneaalifah syarafinaPas encore d'évaluation
- Burn ManagementDocument7 pagesBurn ManagementnrhmhealthPas encore d'évaluation
- S - Radiation and ChemotherapyDocument57 pagesS - Radiation and ChemotherapySusovan GiriPas encore d'évaluation
- Guide To Treatment of Tattoo Complications and Tattoo RemovalDocument7 pagesGuide To Treatment of Tattoo Complications and Tattoo RemovalDannyPas encore d'évaluation
- Burn InjuriesDocument30 pagesBurn InjuriesIndra PrasetyaPas encore d'évaluation
- Pavlidis 2016Document14 pagesPavlidis 2016igorfragaPas encore d'évaluation
- Effective Treatment of Rosacea Using Intense Pulsed LightDocument5 pagesEffective Treatment of Rosacea Using Intense Pulsed LightVo Ha Phuong NguyenPas encore d'évaluation
- Topical Corticosteroid AbuseDocument34 pagesTopical Corticosteroid AbuseDr Daulat Ram DhakedPas encore d'évaluation
- Dermatology For The General SurgeonDocument24 pagesDermatology For The General SurgeonAnita HerreraPas encore d'évaluation
- Burns An Introduction To Burns and Basic Wound - 2023 - Physician Assistant CliDocument11 pagesBurns An Introduction To Burns and Basic Wound - 2023 - Physician Assistant CliJose AnaconaPas encore d'évaluation
- UWorld Medicine - Paeds - Surgery (COMPLETE)Document226 pagesUWorld Medicine - Paeds - Surgery (COMPLETE)abdulmoiz92100% (1)
- Elton 1983Document7 pagesElton 1983Laura GarciaPas encore d'évaluation
- Burn Injuries and Management - Dr. Ihab AzzamDocument12 pagesBurn Injuries and Management - Dr. Ihab Azzambiii boooPas encore d'évaluation
- Burns ClassificationDocument4 pagesBurns ClassificationNedaAbdullahPas encore d'évaluation
- Actinic KeratosesDocument3 pagesActinic KeratosesRenata MeloPas encore d'évaluation
- Chapter 57Document10 pagesChapter 572071317Pas encore d'évaluation
- Topical Issues in DermatologyDocument8 pagesTopical Issues in DermatologyRohini SelvarajahPas encore d'évaluation
- Medicina 58 00115Document12 pagesMedicina 58 00115satriaPas encore d'évaluation
- Daylight Photodynamic Therapy For The Treatment of Actinic CheilitisDocument6 pagesDaylight Photodynamic Therapy For The Treatment of Actinic CheilitisNamiraPas encore d'évaluation
- Management of Keloids and Hypertrophic Scars Current Anf Emerging OptionsDocument12 pagesManagement of Keloids and Hypertrophic Scars Current Anf Emerging OptionsCyntia RatnadiPas encore d'évaluation
- Standard Guidelines of Care - Keloids and Hypertrophic Scars (Somesh Gupta VK Sharma)Document8 pagesStandard Guidelines of Care - Keloids and Hypertrophic Scars (Somesh Gupta VK Sharma)AuroraPas encore d'évaluation
- BurnsDocument106 pagesBurnsShahini PrajapatiPas encore d'évaluation
- Terjemahan KulitDocument5 pagesTerjemahan KulitErlieza Rosdania SupraptoPas encore d'évaluation
- Plastic Surgery SummaryDocument30 pagesPlastic Surgery SummaryLailaAliPas encore d'évaluation
- BurnDocument44 pagesBurnyohannesPas encore d'évaluation
- Perioral Dermatitis - StatPearls - NCBI BookshelfDocument5 pagesPerioral Dermatitis - StatPearls - NCBI BookshelfHanna ABPas encore d'évaluation
- Burns Management PDFDocument7 pagesBurns Management PDFRoh Bungaria N Garingging100% (1)
- Webinar Argano Melasma and Januluma DR Seraj Nonpharmacologic ManagementDocument22 pagesWebinar Argano Melasma and Januluma DR Seraj Nonpharmacologic Managementmohammad kazem HajianiPas encore d'évaluation
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Treatment of Severe Drug ReactionsDocument8 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Treatment of Severe Drug ReactionsHaidir MuhammadPas encore d'évaluation
- Procedures Skin Tag RemovalDocument5 pagesProcedures Skin Tag RemovalIrvan Dwi FitraPas encore d'évaluation
- Treatment of Minor Thermal BurnsDocument22 pagesTreatment of Minor Thermal BurnsTP RMad100% (1)
- The White Army-BurnsDocument69 pagesThe White Army-BurnsVishnu PriyaPas encore d'évaluation
- Localized Acneiform Eruption Induced by Radiation Therapy: Case ReportDocument2 pagesLocalized Acneiform Eruption Induced by Radiation Therapy: Case ReportDwi Esthi PutriPas encore d'évaluation
- Burns and Wound Healing PDFDocument6 pagesBurns and Wound Healing PDFJorge De VeraPas encore d'évaluation
- Clinical Review - FullDocument5 pagesClinical Review - FullAnen LightPas encore d'évaluation
- Burns - Infection, Risk ForDocument4 pagesBurns - Infection, Risk Formakyofrancis20Pas encore d'évaluation
- Acute Wound CareDocument73 pagesAcute Wound CareDikaPas encore d'évaluation
- Acne Scars: Subcision: Methods and TechniquesDocument3 pagesAcne Scars: Subcision: Methods and TechniquesLuiz Henrique CararetoPas encore d'évaluation
- 7417 Skin Tag RemovalDocument4 pages7417 Skin Tag RemovalNikolaus TalloPas encore d'évaluation
- PsoriasisDocument40 pagesPsoriasisAmrit Preet KaurPas encore d'évaluation
- Facial Skin Rejuvenation: Ablative Laser Resurfacing, Chemical Peels, or Photodynamic Therapy? Facts and ControversiesDocument4 pagesFacial Skin Rejuvenation: Ablative Laser Resurfacing, Chemical Peels, or Photodynamic Therapy? Facts and ControversiesCarlla Araújo Guarani KaiowáPas encore d'évaluation
- Laser Treatment For Post Acne Scars - A ReviewDocument6 pagesLaser Treatment For Post Acne Scars - A ReviewAryantii AntyPas encore d'évaluation
- Burns Assessment - TeachMeSurgeryDocument5 pagesBurns Assessment - TeachMeSurgeryLaroui HoPas encore d'évaluation
- Burn Management PDFDocument7 pagesBurn Management PDFMuhammad huseinPas encore d'évaluation
- Management of Wound InfectionDocument7 pagesManagement of Wound InfectionRoza LiaaPas encore d'évaluation
- Modern Wound Care Practical Aspects of Non Interventional Topical Treatment of Patients With Chronic WoundsDocument14 pagesModern Wound Care Practical Aspects of Non Interventional Topical Treatment of Patients With Chronic WoundsDauz ArashPas encore d'évaluation
- Innovative Biochemisurgical Treatment For Stabilisat 2024 International JourDocument6 pagesInnovative Biochemisurgical Treatment For Stabilisat 2024 International JourRonald QuezadaPas encore d'évaluation
- Pedo 2016-18 PDFDocument4 pagesPedo 2016-18 PDFJude Aldo PaulPas encore d'évaluation
- HemiglossectomyDocument3 pagesHemiglossectomyKraftchezPas encore d'évaluation
- History of LaparosDocument27 pagesHistory of LaparosDr. Sanjay KoltePas encore d'évaluation
- Research EssayDocument7 pagesResearch EssayAkashdeep SinghPas encore d'évaluation
- Otolaryngology MCQ: 2009july 12, 2009Document60 pagesOtolaryngology MCQ: 2009july 12, 2009Ali QuwarahPas encore d'évaluation
- ConnectiCare Bronze StandardDocument98 pagesConnectiCare Bronze Standardalex647Pas encore d'évaluation
- A Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsDocument6 pagesA Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsTeresaPas encore d'évaluation
- 3161 9711 1 SMDocument3 pages3161 9711 1 SMpuskesmas sidosermoPas encore d'évaluation
- Prospectus New India Floater Mediclaim Wef 01 04 2021Document26 pagesProspectus New India Floater Mediclaim Wef 01 04 2021SnehaAnilSurvePas encore d'évaluation
- Health Care Delivery System 1Document21 pagesHealth Care Delivery System 1Carson BirthPas encore d'évaluation
- Special Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40Document21 pagesSpecial Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40tobyPas encore d'évaluation
- Hyperthermia HIV NURSING CARE PLAN FLODocument4 pagesHyperthermia HIV NURSING CARE PLAN FLOMicaela CrisostomoPas encore d'évaluation
- The Caregiver Training CurriculumDocument10 pagesThe Caregiver Training CurriculumOlaya alghareniPas encore d'évaluation
- Protocol of Radiotherapy For Rectal CancerDocument3 pagesProtocol of Radiotherapy For Rectal CancerValentino PetrePas encore d'évaluation
- The Front Desk: NABH Quality Management For Rural HospitalsDocument6 pagesThe Front Desk: NABH Quality Management For Rural HospitalsMehar AwaisPas encore d'évaluation
- Neutral Zone Concept and Its Technique at Impression Stage PDFDocument7 pagesNeutral Zone Concept and Its Technique at Impression Stage PDFgeneral generalPas encore d'évaluation
- Ethical and Legal Issues in Midwifery and ObstetricsDocument9 pagesEthical and Legal Issues in Midwifery and ObstetricsMahenur100% (2)
- Concept Map Paper Steve NaraineDocument6 pagesConcept Map Paper Steve Naraineapi-283596053Pas encore d'évaluation
- Ambulatory Care Medical Surgical NursingDocument11 pagesAmbulatory Care Medical Surgical NursingNiña Antoniette Gutang100% (4)
- DR Shoaib S Khan - CV - ResumeDocument2 pagesDR Shoaib S Khan - CV - ResumeEmaad IshakPas encore d'évaluation
- Guideline On Provisional Certifiaction As Primary Care Provider For FCM ResidentsDocument2 pagesGuideline On Provisional Certifiaction As Primary Care Provider For FCM ResidentsJames Lagamayo JavierPas encore d'évaluation
- Cigna Dental Care Patient Charge Schedule: (Dhmo)Document16 pagesCigna Dental Care Patient Charge Schedule: (Dhmo)Susanta BeheraPas encore d'évaluation
- Minggu I Miftahul Rauhan Bedah Plastik Ulkus DekubitusDocument25 pagesMinggu I Miftahul Rauhan Bedah Plastik Ulkus DekubitusmiftahulrauhanPas encore d'évaluation
- Human Factors and Ergonomics in Health Care and Patient SafetyDocument35 pagesHuman Factors and Ergonomics in Health Care and Patient SafetymourtiPas encore d'évaluation
- Odb CdiDocument644 pagesOdb CdiPaul JagdharryPas encore d'évaluation
- UNIT 1A. Assessing Community NeedsDocument116 pagesUNIT 1A. Assessing Community NeedsSebastianPas encore d'évaluation
- How To Calculate Calories Intake: by Group 6Document9 pagesHow To Calculate Calories Intake: by Group 6Reina Magfirah MokogintaPas encore d'évaluation
- NCP of Fever and HypertensionDocument2 pagesNCP of Fever and HypertensionDayan CabrigaPas encore d'évaluation
- Advanced Vol22n15Document65 pagesAdvanced Vol22n15Anderson Japa RibeiroPas encore d'évaluation
- BW Health-5Document2 pagesBW Health-5Michael JaballasPas encore d'évaluation
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4 sur 5 étoiles4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryD'EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryÉvaluation : 4 sur 5 étoiles4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerD'EverandGut: the new and revised Sunday Times bestsellerÉvaluation : 4 sur 5 étoiles4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisD'EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- The Marshmallow Test: Mastering Self-ControlD'EverandThe Marshmallow Test: Mastering Self-ControlÉvaluation : 4.5 sur 5 étoiles4.5/5 (58)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingD'EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingÉvaluation : 4 sur 5 étoiles4/5 (1138)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningD'EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningÉvaluation : 4 sur 5 étoiles4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessD'EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (328)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsD'EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsÉvaluation : 4.5 sur 5 étoiles4.5/5 (6)