Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Male Genital ExaminationDocument4 pagesThe Male Genital ExaminationNiala AlmarioPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- U.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3Document5 pagesU.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3mtataPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Dr. Ali's Uworld Notes For Step 2 CKDocument30 pagesDr. Ali's Uworld Notes For Step 2 CKuyesPas encore d'évaluation
- Screening Guidelines For Primary CareDocument143 pagesScreening Guidelines For Primary CareMiguelinda V Kim89% (19)
- First Aid For The Family Medicine Boards Third Edition 1st TheDocument61 pagesFirst Aid For The Family Medicine Boards Third Edition 1st Thejerry.wolff991100% (39)
- 2014 BRE IndianapolisDocument3 495 pages2014 BRE IndianapolisIan ScottPas encore d'évaluation
- Mens Health ChecklistDocument4 pagesMens Health Checklistglobalmark100% (1)
- Gerontologic NursingDocument231 pagesGerontologic NursingKirk08100% (2)
- The Current Evidence-Based Medicine LandscapeDocument140 pagesThe Current Evidence-Based Medicine LandscapeNational Pharmaceutical Council88% (8)
- The Already Dead by Eric CazdynDocument16 pagesThe Already Dead by Eric CazdynDuke University Press100% (1)
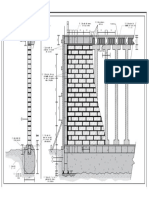
- Entrega de Albañileria Confinada-Presentación1Document1 pageEntrega de Albañileria Confinada-Presentación1AdolfoDavidPas encore d'évaluation
- Entrega de Albañileria Confinada-ModeloDocument1 pageEntrega de Albañileria Confinada-ModeloAdolfoDavidPas encore d'évaluation
- Cepunc - Módulo BDocument6 pagesCepunc - Módulo BAdolfoDavidPas encore d'évaluation
- Advanced CalculusDocument592 pagesAdvanced Calculusjosemarcelod7088Pas encore d'évaluation
- SadfasdfDocument1 pageSadfasdfAdolfoDavidPas encore d'évaluation
- SadfasdfDocument1 pageSadfasdfAdolfoDavidPas encore d'évaluation
- National - Guideline A4 Final PDFDocument56 pagesNational - Guideline A4 Final PDFOsama AlmuqrinPas encore d'évaluation
- USPSTF Screening Recommendations (Across The Ages)Document8 pagesUSPSTF Screening Recommendations (Across The Ages)Jessica MoorePas encore d'évaluation
- Breast Cancer ScreeningDocument9 pagesBreast Cancer Screeningsorin.morosan64Pas encore d'évaluation
- Columbia University Health Insurance ProspectusDocument46 pagesColumbia University Health Insurance ProspectusAlva FRENCH-N'GUESSANPas encore d'évaluation
- Gynecology Screening ProceduresDocument30 pagesGynecology Screening Proceduresapi-506496190Pas encore d'évaluation
- Delay SpeechDocument8 pagesDelay Speechshrt gtPas encore d'évaluation
- Preventive Task ForceDocument2 pagesPreventive Task ForceRocioBeteluPas encore d'évaluation
- Turkey BK 2013 - Full VersionDocument147 pagesTurkey BK 2013 - Full VersionmmmmzPas encore d'évaluation
- Death by AbleismDocument3 pagesDeath by AbleismtolliPas encore d'évaluation
- Do Younger Women Need MammogramsDocument5 pagesDo Younger Women Need MammogramsjohntandraPas encore d'évaluation
- Diagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATADocument61 pagesDiagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATAtabhsinghiPas encore d'évaluation
- LifeextensionDocument84 pagesLifeextensionhermestriPas encore d'évaluation
- USPSTF A and B RecomendationsDocument5 pagesUSPSTF A and B RecomendationsVishala MishraPas encore d'évaluation
- Evidence-Based Labor and Delivery Management PDFDocument10 pagesEvidence-Based Labor and Delivery Management PDFmadeemjPas encore d'évaluation
- National Guideline Clearinghouse PortalDocument4 pagesNational Guideline Clearinghouse PortalValerie R. HoughtonPas encore d'évaluation
- Annotated BibliographyDocument3 pagesAnnotated Bibliographyapi-252346228Pas encore d'évaluation
- Breast Cancer Epidemiology, StellaDocument32 pagesBreast Cancer Epidemiology, StellaLamchabbek NajouaPas encore d'évaluation
- National Periodic Health GuidelinesDocument72 pagesNational Periodic Health Guidelinesasma .sassiPas encore d'évaluation
- Tamizaje Ca de PulmonDocument11 pagesTamizaje Ca de Pulmonjuan CARLOS vaRGASPas encore d'évaluation
- Suicidal Ideation and Behavior in Adults - UpToDate PDFDocument36 pagesSuicidal Ideation and Behavior in Adults - UpToDate PDFLemuel ReyesPas encore d'évaluation