Vous aimerez peut-être aussi
- Evidence Based PracticeDocument14 pagesEvidence Based PracticeKrini Tandel100% (2)
- Evidence Based Practice: 5) Case Reports and Clinical ExamplesDocument11 pagesEvidence Based Practice: 5) Case Reports and Clinical ExamplesSahaj Yadav100% (5)
- Evidence-Based Nursing PracticeDocument12 pagesEvidence-Based Nursing PracticeJaylen Cay100% (6)
- Evidence Based Nursing PracticeDocument15 pagesEvidence Based Nursing PracticeMuhammad Abifurqon Habibi100% (2)
- ANP - EBP Model ASHDocument12 pagesANP - EBP Model ASHManoj BalaPas encore d'évaluation
- Evidence Based Practice FinalDocument22 pagesEvidence Based Practice Finalgopscharan100% (1)
- Evidence Based Practice in Nursing BinuDocument51 pagesEvidence Based Practice in Nursing BinuBinu Joshva100% (3)
- Evidence Based PracticeDocument18 pagesEvidence Based PracticeAmanda Scarlet100% (2)
- Assignment of AnpDocument18 pagesAssignment of Anpcharanjit kaurPas encore d'évaluation
- EBNPDocument62 pagesEBNPShailja Sharma100% (1)
- Framework Trend and Scope of Nursing PracticeDocument28 pagesFramework Trend and Scope of Nursing PracticeShaells Joshi80% (5)
- Futuristic Nursing: - Sister Elizabeth DavisDocument14 pagesFuturistic Nursing: - Sister Elizabeth DavisPhebeDimple100% (2)
- Expanded and Extended Role of NurseDocument31 pagesExpanded and Extended Role of Nurserajeshwari83% (18)
- Human Resource For HealthDocument19 pagesHuman Resource For HealthUdaya Sree100% (3)
- Futuristic NursingDocument15 pagesFuturistic Nursingmanu sethi79% (19)
- Peplaus TheoryDocument17 pagesPeplaus Theorydanimon1984Pas encore d'évaluation
- Innovation in Nursing CurrentDocument30 pagesInnovation in Nursing Currentbemina jaPas encore d'évaluation
- Health Education BureauDocument13 pagesHealth Education Bureauv_vijayakanth7656Pas encore d'évaluation
- Futuristic Nursing PDFDocument39 pagesFuturistic Nursing PDFRudra prasad SahuPas encore d'évaluation
- Sensory Deprivation.Document7 pagesSensory Deprivation.KJ Bindu100% (1)
- Current Trends in Nursing Educaion..MadhuDocument13 pagesCurrent Trends in Nursing Educaion..Madhuprecillathoppil100% (1)
- Dvance Ursing Ractice: Seminar ON Professional Organizations, Unions and Self DefenceDocument19 pagesDvance Ursing Ractice: Seminar ON Professional Organizations, Unions and Self DefenceValarmathiPas encore d'évaluation
- Evidence Based Practice ModelDocument81 pagesEvidence Based Practice ModelNancy Singh100% (4)
- Long Seminar: Computer Application For Patient Care Delivery System and Nursing PracticeDocument18 pagesLong Seminar: Computer Application For Patient Care Delivery System and Nursing Practicepandem soniya100% (2)
- Innovations in NursingDocument14 pagesInnovations in Nursingrizwan33% (3)
- Nursing Advocacy PPT Case StudyDocument10 pagesNursing Advocacy PPT Case StudyFitria Ananda PutriPas encore d'évaluation
- Seminar On Dual Role of NurseDocument16 pagesSeminar On Dual Role of Nursedanimon198475% (4)
- StakeholderDocument57 pagesStakeholderpandem soniyaPas encore d'évaluation
- Innovations in NursingDocument13 pagesInnovations in NursingShubha JeniferPas encore d'évaluation
- Patterns of Nursing Care DeliveryDocument32 pagesPatterns of Nursing Care DeliveryJayarani Ashok0% (1)
- Edu ReformDocument17 pagesEdu ReformNikita NelsonPas encore d'évaluation
- Scope of Nursing ResearchDocument16 pagesScope of Nursing Researchvincy100% (6)
- Homeostatic, Biological and Psychodynamics in Disease CausationDocument5 pagesHomeostatic, Biological and Psychodynamics in Disease CausationMeenu Dogra100% (1)
- Faculty Relationship RAVINDRA SEM 2Document11 pagesFaculty Relationship RAVINDRA SEM 2Mallika Joon100% (1)
- MiesDocument40 pagesMiessanthiyasandyPas encore d'évaluation
- Evidence Based Practice ModelsDocument76 pagesEvidence Based Practice ModelsLIDIYA MOL P V86% (7)
- Educational Aims and Objectives-2Document22 pagesEducational Aims and Objectives-2Shruthi Pingula100% (2)
- Application of Nursing Theory of Dorothea Orem WRDDocument26 pagesApplication of Nursing Theory of Dorothea Orem WRDLIDIYA MOL P V100% (5)
- Independent Practice IssuesDocument7 pagesIndependent Practice IssuesPradip Chougale100% (5)
- Visit To PSG College of Nursing: Submitted To Submitted byDocument8 pagesVisit To PSG College of Nursing: Submitted To Submitted byShubha JeniferPas encore d'évaluation
- Extended and Expanded Roles of Nurse AnpDocument11 pagesExtended and Expanded Roles of Nurse AnpSamjhana Neupane0% (1)
- Competency Based Education & OutcomeDocument24 pagesCompetency Based Education & OutcomeArchana Sahu100% (2)
- Futuristic NursingDocument14 pagesFuturistic NursingHarpreet Dhatt50% (4)
- Nurses Role Organ DonationDocument11 pagesNurses Role Organ DonationKrishna TejavathPas encore d'évaluation
- Annotated BibliographyDocument18 pagesAnnotated BibliographyBriana Pierre67% (3)
- Peplau's Interpersonal Relations Theory Power PointDocument10 pagesPeplau's Interpersonal Relations Theory Power PointPerlie Loren Arreo Cabatingan100% (1)
- Antenatal Aspect Preventive PeadiarricsDocument28 pagesAntenatal Aspect Preventive PeadiarricsYashoda SatputePas encore d'évaluation
- School of Nursing Science and Research (Sharda University) : Assignment ON Alternative Modalities of CareDocument13 pagesSchool of Nursing Science and Research (Sharda University) : Assignment ON Alternative Modalities of CareSamjhana Neupane100% (1)
- Assignment On Historcal Evolution of Research in NursingDocument35 pagesAssignment On Historcal Evolution of Research in NursingPoonam Dhatwalia100% (1)
- Innovations in NursingDocument14 pagesInnovations in NursingDelphy Varghese100% (1)
- Power and Politics in NursingDocument14 pagesPower and Politics in NursingRufus Raj100% (2)
- Nursing Practice Framework Scope and TrendsDocument9 pagesNursing Practice Framework Scope and TrendsAru Verma100% (3)
- FY MSC Community Health Nursing Clinical Specialty IDocument4 pagesFY MSC Community Health Nursing Clinical Specialty IPriya Sharma100% (1)
- Application of OremDocument19 pagesApplication of OremBhekti ImansariPas encore d'évaluation
- Advanced Practice RolesDocument16 pagesAdvanced Practice RolesLorelie Asis0% (1)
- Oxygen InsufficiencyDocument24 pagesOxygen InsufficiencyAnusha VerghesePas encore d'évaluation
- Continuing Nursing EducationDocument30 pagesContinuing Nursing EducationSalim MusthafaPas encore d'évaluation
- Class Presentation On Evaluation Strategies & Process of Curriculum ChangeDocument5 pagesClass Presentation On Evaluation Strategies & Process of Curriculum Changemadhurima kundu100% (2)
- CardiacDocument37 pagesCardiacmeghanaPas encore d'évaluation
- Adult Health PerfomaDocument2 pagesAdult Health PerfomameghanaPas encore d'évaluation
- Pre and Postoperative CareDocument17 pagesPre and Postoperative CaremeghanaPas encore d'évaluation
- Guillain Barre Syndrome-PPT FinalDocument39 pagesGuillain Barre Syndrome-PPT Finalmeghana100% (1)
- Women EmpowermentDocument11 pagesWomen Empowermentmeghana100% (2)
- Health AssessmentDocument15 pagesHealth AssessmentmeghanaPas encore d'évaluation
- Indian Constitution: Mrs. Meghana Goswami 2 Year M.SC NursingDocument19 pagesIndian Constitution: Mrs. Meghana Goswami 2 Year M.SC Nursingmeghana100% (1)
- Health Talk - Diet in AnemiaDocument17 pagesHealth Talk - Diet in Anemiameghana88% (8)
- Manibabhula Nursing College, Bardoli: Subject: Medical Surgical Nursing Topic: Case Study OnDocument18 pagesManibabhula Nursing College, Bardoli: Subject: Medical Surgical Nursing Topic: Case Study Onmeghana100% (4)
- Maniba Bhula Nursing College: Subject: TopicDocument11 pagesManiba Bhula Nursing College: Subject: TopicmeghanaPas encore d'évaluation
- Ms. Meghana Goswami 1 Year M.SC M.B.N.CDocument12 pagesMs. Meghana Goswami 1 Year M.SC M.B.N.CmeghanaPas encore d'évaluation
- Administration Presentation..Fre..1Document6 pagesAdministration Presentation..Fre..1meghana100% (1)
- TuberculosisDocument17 pagesTuberculosismeghana100% (2)
- Inventory Control: Inventory Management Is A Great Time-Saving Tool. We Can Save The Time byDocument8 pagesInventory Control: Inventory Management Is A Great Time-Saving Tool. We Can Save The Time bymeghanaPas encore d'évaluation
- BronchitisDocument24 pagesBronchitismeghana67% (3)
- Maniba Bhula Nursing College: Subject: TopicDocument20 pagesManiba Bhula Nursing College: Subject: Topicmeghana100% (1)
- Angina (Coronary Artery Disease/Acute Coronary Syndrome) : Care SettingDocument17 pagesAngina (Coronary Artery Disease/Acute Coronary Syndrome) : Care SettingmeghanaPas encore d'évaluation
- Budget Estimate, Revised Estimate, Performance BudgetDocument7 pagesBudget Estimate, Revised Estimate, Performance Budgetmeghana0% (2)
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument46 pagesCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaPas encore d'évaluation
- Intestinal Obstruction, Colorectal CancerDocument49 pagesIntestinal Obstruction, Colorectal CancermeghanaPas encore d'évaluation
- Ms. Meghana Goswami 1 Year M.Sc. Student M.B.N.CDocument11 pagesMs. Meghana Goswami 1 Year M.Sc. Student M.B.N.CmeghanaPas encore d'évaluation
- ArchanaDocument6 pagesArchanaArchana DeviPas encore d'évaluation
- IMRAD Tabo VendorsDocument8 pagesIMRAD Tabo VendorsEarly Joy BorjaPas encore d'évaluation
- Students Satisfaction On Byju'S Learning App: Project Report Submitted ToDocument75 pagesStudents Satisfaction On Byju'S Learning App: Project Report Submitted ToHemant Deshmukh100% (1)
- Indian Ethos and Values: by DR Kishor BaradDocument26 pagesIndian Ethos and Values: by DR Kishor BaradAalap N PrajapatiPas encore d'évaluation
- Study Plan Template 32Document6 pagesStudy Plan Template 32Abdul TawabPas encore d'évaluation
- Chapter 12 - SummaryDocument2 pagesChapter 12 - SummaryHồ NguyễnPas encore d'évaluation
- Project Title:-Impact of Celebrity Endorsement On Buying Behavior of Consumers and Source of Brand Building AbstractDocument9 pagesProject Title:-Impact of Celebrity Endorsement On Buying Behavior of Consumers and Source of Brand Building AbstractRajesh InsbPas encore d'évaluation
- Group Assignment 2: SB2023 Dr. Le Anh TuanDocument2 pagesGroup Assignment 2: SB2023 Dr. Le Anh TuanHuyen cao thi thanhPas encore d'évaluation
- 01 - Multivariate - Introduction To Multivariate AnalysisDocument38 pages01 - Multivariate - Introduction To Multivariate Analysis322OO22 - Jovanka Angella Mesinay100% (1)
- Poulsen Khanal Waste DumpDocument14 pagesPoulsen Khanal Waste DumpWangga SebayangPas encore d'évaluation
- Application Form For Registration of Herbal and Complementary Medicine - 1Document4 pagesApplication Form For Registration of Herbal and Complementary Medicine - 1roykibetPas encore d'évaluation
- MBCT P ManualDocument18 pagesMBCT P ManualAnonymous VYzPQ9vtPas encore d'évaluation
- Business - June 2023 Examiners Report (2r)Document49 pagesBusiness - June 2023 Examiners Report (2r)Rayyan BabarPas encore d'évaluation
- Mobile Money Adoption in A Fragile Economy: The Case of A Seven Year Failed Experiment in NigeriaDocument10 pagesMobile Money Adoption in A Fragile Economy: The Case of A Seven Year Failed Experiment in NigeriainventionjournalsPas encore d'évaluation
- Business Analyst Resume TemplateDocument8 pagesBusiness Analyst Resume Templatekqgcnxejd100% (2)
- 4.3 Components of A Research ProposalDocument7 pages4.3 Components of A Research ProposalROGEN MAE DIONIOPas encore d'évaluation
- Advocacy in The Customer Focused Enterprise - IBM PDFDocument28 pagesAdvocacy in The Customer Focused Enterprise - IBM PDFAlberto ConzPas encore d'évaluation
- An Overview of The Schwartz Theory of Basic ValuesDocument20 pagesAn Overview of The Schwartz Theory of Basic ValuesTaufiq Adi WijayaPas encore d'évaluation
- Millat Tractor: Auto Mobile Agriculture IndustryDocument27 pagesMillat Tractor: Auto Mobile Agriculture IndustryZaman RanaPas encore d'évaluation
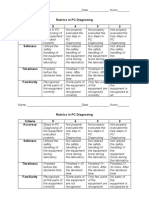
- Rubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - ScoreDocument2 pagesRubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - Scorejhun ecleoPas encore d'évaluation
- A Taxonomy of Ecodesign Tools For Integrating Environmental Requirements Into The Product Design ProcessDocument11 pagesA Taxonomy of Ecodesign Tools For Integrating Environmental Requirements Into The Product Design ProcessJ.C.VPas encore d'évaluation
- 4ps of MarketingDocument2 pages4ps of MarketingCLLN FILESPas encore d'évaluation
- Session3 Emp-Res M11-HRM Was 5hrmDocument26 pagesSession3 Emp-Res M11-HRM Was 5hrmUrsuline Egbulem100% (1)
- Class 9Document15 pagesClass 9Diya lizbeth josePas encore d'évaluation
- The Influence of Gender On Clinical Examination Skills of Medical Students in Jordan: A Cross-Sectional StudyDocument10 pagesThe Influence of Gender On Clinical Examination Skills of Medical Students in Jordan: A Cross-Sectional StudymoPas encore d'évaluation
- Geo Politics FEU PolSciDocument39 pagesGeo Politics FEU PolSciJF DanPas encore d'évaluation
- Chapter 5 Full SolutionsDocument21 pagesChapter 5 Full SolutionsBar AzilaPas encore d'évaluation
- Apqp PDFDocument151 pagesApqp PDFMehul TrivediPas encore d'évaluation
- Writing - Free Writing Short NarrativeDocument11 pagesWriting - Free Writing Short NarrativeSaravana SelvakumarPas encore d'évaluation
- Research Update 1Document57 pagesResearch Update 1Francisco, John Eiyen D.Pas encore d'évaluation