Vous aimerez peut-être aussi
- The Dynamic Law of ProsperityDocument1 pageThe Dynamic Law of Prosperitypapayasmin75% (4)
- Sanogo 2019 TFDocument40 pagesSanogo 2019 TFbassomassi sanogoPas encore d'évaluation
- Precocious PubertyDocument30 pagesPrecocious PubertyAjoritsedere Eric AkonuPas encore d'évaluation
- Summary of Dirty Genes: by Ben Lynch ND. - A Breakthrough Program to Treat the Root Cause of Illness and Optimize Your Health - A Comprehensive SummaryD'EverandSummary of Dirty Genes: by Ben Lynch ND. - A Breakthrough Program to Treat the Root Cause of Illness and Optimize Your Health - A Comprehensive SummaryPas encore d'évaluation
- Puberty: Dr. Valérie M. SchwitzgebelDocument66 pagesPuberty: Dr. Valérie M. SchwitzgebelJoshua RomeroPas encore d'évaluation
- ENDOCRINE NURSING-FINAL HDDocument15 pagesENDOCRINE NURSING-FINAL HDJayvee Novenario Casaljay100% (1)
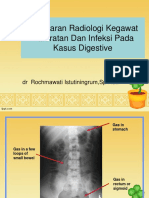
- K29 - Radiologi Blok Digestive 2015Document117 pagesK29 - Radiologi Blok Digestive 2015NininghrPas encore d'évaluation
- Growth and Growth Hormone - An Overview PDFDocument3 pagesGrowth and Growth Hormone - An Overview PDFFajar Yuniftiadi0% (1)
- B. 10 Situation - Care of Client With Problems in Metabolism & Endocrine Functioning.Document7 pagesB. 10 Situation - Care of Client With Problems in Metabolism & Endocrine Functioning.SOLEIL LOUISE LACSON MARBAS100% (1)
- Gyne PcosDocument50 pagesGyne PcosPrecious Medina100% (1)
- Growth Hormone Therapy: Guided By: Dr. Arif VohraDocument45 pagesGrowth Hormone Therapy: Guided By: Dr. Arif VohraMitulPas encore d'évaluation
- System Disorder GHDDocument1 pageSystem Disorder GHDSariahPas encore d'évaluation
- Pemicu 3: Siklus Hidup 2014Document54 pagesPemicu 3: Siklus Hidup 2014exxxxooooPas encore d'évaluation
- New Introduction To Short StatureDocument25 pagesNew Introduction To Short Statureheba1997bshPas encore d'évaluation
- Precocious Puberty: ObjectiveDocument16 pagesPrecocious Puberty: ObjectiveZafar JavedPas encore d'évaluation
- Physiology of Growth and Growth Factors Alrashid SU 2023 AKADocument26 pagesPhysiology of Growth and Growth Factors Alrashid SU 2023 AKARaghad AlPas encore d'évaluation
- Precociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Document31 pagesPrecociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Priya RaviPas encore d'évaluation
- Disorder of Puberty RevisiDocument29 pagesDisorder of Puberty RevisiRamaPas encore d'évaluation
- Disorders of Growth and DevelopmentDocument52 pagesDisorders of Growth and DevelopmentMaria Hudson100% (1)
- Approach To Short StatureDocument71 pagesApproach To Short StatureOmar HamwiPas encore d'évaluation
- Pubertal Disorders LectureDocument60 pagesPubertal Disorders LectureRawabi rawabi1997Pas encore d'évaluation
- The Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewDocument27 pagesThe Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewEdelrose LapitanPas encore d'évaluation
- Short Stature 2Document64 pagesShort Stature 2amit kumarPas encore d'évaluation
- Physical Growth AND Puberty: Aditiawati Division of Pediatric Endocrinology Dept of Child Health FK Unsri-RSMHDocument77 pagesPhysical Growth AND Puberty: Aditiawati Division of Pediatric Endocrinology Dept of Child Health FK Unsri-RSMHAudrey Ira YunitaPas encore d'évaluation
- Growth Hormone Deficiency - ChildrenDocument4 pagesGrowth Hormone Deficiency - ChildrenFenita Renny DinataPas encore d'évaluation
- 8-Acromegaly & DwarfismDocument79 pages8-Acromegaly & DwarfismsweyamkulimaPas encore d'évaluation
- Precocious PubertyDocument30 pagesPrecocious PubertyNeha SharmaPas encore d'évaluation
- Precocious Puberty 1Document14 pagesPrecocious Puberty 1RenPas encore d'évaluation
- The Hypothalamic-Pituitary-Endocrine AxisDocument46 pagesThe Hypothalamic-Pituitary-Endocrine Axiskaleab AlemayehuPas encore d'évaluation
- Endo Part IVDocument40 pagesEndo Part IVChippy RabePas encore d'évaluation
- EMS Case 1 MPHDDocument44 pagesEMS Case 1 MPHDFatita Restu HermawanPas encore d'évaluation
- Understanding Puberty: Physical Changes and Hormonal DevelopmentDocument66 pagesUnderstanding Puberty: Physical Changes and Hormonal DevelopmentnenyPas encore d'évaluation
- Puberty PDFDocument66 pagesPuberty PDFnenyPas encore d'évaluation
- Puberty: Dr. Valérie M. SchwitzgebelDocument66 pagesPuberty: Dr. Valérie M. SchwitzgebelnenyPas encore d'évaluation
- Unit IV CompleteDocument116 pagesUnit IV CompleteAlok RanjanPas encore d'évaluation
- Growth Hormone Deficiency - A Case ReportDocument3 pagesGrowth Hormone Deficiency - A Case ReportAyiek WicaksonoPas encore d'évaluation
- Short Stature: - CausesDocument18 pagesShort Stature: - CausesYusri ArifPas encore d'évaluation
- Minutes) Everybody WritesDocument15 pagesMinutes) Everybody WritesRanes AndyPas encore d'évaluation
- Growth Hormone DeficiencyDocument11 pagesGrowth Hormone DeficiencyIgor VasićPas encore d'évaluation
- 1 Endocrinology 1Document14 pages1 Endocrinology 1Jessa MayPas encore d'évaluation
- ArainDocument71 pagesArainAllah Bux KhosoPas encore d'évaluation
- Pediatrics - Endocrine System (Part1)Document150 pagesPediatrics - Endocrine System (Part1)Gen XPas encore d'évaluation
- Pituitary, Thyroid & Adrenal HormonesDocument13 pagesPituitary, Thyroid & Adrenal HormonesJose Melmar Autida AutenticoPas encore d'évaluation
- Reproduction Block (Puberty) Khairun Nisa Bagian Fisiologi FK Unila 216Document28 pagesReproduction Block (Puberty) Khairun Nisa Bagian Fisiologi FK Unila 216Redina AndiniPas encore d'évaluation
- Pediatric Growth Hormone Deficiency GuideDocument15 pagesPediatric Growth Hormone Deficiency GuideEdinson Cabrera MenesesPas encore d'évaluation
- Anatomy & Physiology of Precocious PubertyDocument19 pagesAnatomy & Physiology of Precocious PubertyAshlene Kate BagsiyaoPas encore d'évaluation
- 02 Kuliah Semester VI - 2011 - 1Document40 pages02 Kuliah Semester VI - 2011 - 1almahdy25051976Pas encore d'évaluation
- CA2018PPt NewDocument32 pagesCA2018PPt NewAshlene Kate BagsiyaoPas encore d'évaluation
- 1 - Short StatureDocument45 pages1 - Short StatureAmmar AlnajjarPas encore d'évaluation
- Growth Hormone, Insulin-like Growth Factor 1 (IGF-1), and their Roles in Growth and MetabolismDocument4 pagesGrowth Hormone, Insulin-like Growth Factor 1 (IGF-1), and their Roles in Growth and MetabolismAisle Malibiran PalerPas encore d'évaluation
- Central Precocious Puberty: Revisiting The Diagnosis and Therapeutic ManagementDocument11 pagesCentral Precocious Puberty: Revisiting The Diagnosis and Therapeutic ManagementRESIDENCIA PEDIATRIAPas encore d'évaluation
- Lecture Notes in Medical Technology - Lecture #2 - The Pituitary Gland - The AdenohypophysisDocument23 pagesLecture Notes in Medical Technology - Lecture #2 - The Pituitary Gland - The AdenohypophysisKat JornadalPas encore d'évaluation
- Precocious PubertyDocument22 pagesPrecocious Pubertywizborrlyzo006Pas encore d'évaluation
- A Review of GrowthDocument8 pagesA Review of GrowthEmilia Diana IacobPas encore d'évaluation
- Hypogonadotropic Hypogonadism: Causes, Diagnosis, and TreatmentDocument14 pagesHypogonadotropic Hypogonadism: Causes, Diagnosis, and TreatmentPrasanth VarghesePas encore d'évaluation
- Physical Growth and Development During AdolescenceDocument54 pagesPhysical Growth and Development During AdolescencereemmajzoubPas encore d'évaluation
- Principles of endocrinology scope and functionsDocument25 pagesPrinciples of endocrinology scope and functionsRyan James Lorenzo MiguelPas encore d'évaluation
- EN18 - Pubertal Development and Male HypogonadismDocument27 pagesEN18 - Pubertal Development and Male Hypogonadismsbobine.imsPas encore d'évaluation
- Hormonal Agents PharmacologyDocument64 pagesHormonal Agents Pharmacologynica velanoPas encore d'évaluation
- Hormonas HipofisariasDocument58 pagesHormonas Hipofisariasitaliaman100% (1)
- Hypothalamus and Pituitary - Physiology and Pathophysiology: Eric J. Epstein, MD Disclosures: NoneDocument49 pagesHypothalamus and Pituitary - Physiology and Pathophysiology: Eric J. Epstein, MD Disclosures: NoneSøren KierkegaardPas encore d'évaluation
- Growth Hormone in Child Growth DisordersDocument44 pagesGrowth Hormone in Child Growth DisordersBayu KurniawanPas encore d'évaluation
- 5-HTP - The Complete Guide - Exploring Its Therapeutic Potential In Depression, Anxiety, Insomnia, And Much More - Benefits, Side Effects, And Scientific Evidence For Human HealthD'Everand5-HTP - The Complete Guide - Exploring Its Therapeutic Potential In Depression, Anxiety, Insomnia, And Much More - Benefits, Side Effects, And Scientific Evidence For Human HealthPas encore d'évaluation
- K47. Vit D and HiperinsulinDocument15 pagesK47. Vit D and HiperinsulinTitisPas encore d'évaluation
- Treating Hansen's Disease: Diagnosis and ManagementDocument16 pagesTreating Hansen's Disease: Diagnosis and ManagementTitisPas encore d'évaluation
- The Classification of Outcome Following Whiplash InjuryDocument5 pagesThe Classification of Outcome Following Whiplash InjuryTitisPas encore d'évaluation
- Short Stature or StuntingDocument16 pagesShort Stature or StuntingTitisPas encore d'évaluation
- Type 1 Diabetes MellitusDocument18 pagesType 1 Diabetes MellitusTitisPas encore d'évaluation
- Disease Occurrence ComparisonDocument12 pagesDisease Occurrence ComparisonTitisPas encore d'évaluation
- Corneal Ulcers WHO PDFDocument36 pagesCorneal Ulcers WHO PDFAlifa FaradillaPas encore d'évaluation
- Kelainan Saraf KongenitalDocument35 pagesKelainan Saraf KongenitalTitisPas encore d'évaluation
- Psikologi BencanaDocument19 pagesPsikologi BencanaTitisPudyatikaDestyaAndiraPas encore d'évaluation
- Pathology of Joints & Related Structure (Dr. Dody) SendiDocument30 pagesPathology of Joints & Related Structure (Dr. Dody) SendiTitisPas encore d'évaluation
- Epidemiology MASDocument1 pageEpidemiology MASTitisPas encore d'évaluation
- DFSGDFGDFDocument60 pagesDFSGDFGDFMada Dwi HariPas encore d'évaluation
- Muscoletalsceletal InjuriesDocument15 pagesMuscoletalsceletal InjuriesTitisPas encore d'évaluation
- Bible TabsDocument8 pagesBible TabsAstrid TabordaPas encore d'évaluation
- Rizal's First Return Home to the PhilippinesDocument52 pagesRizal's First Return Home to the PhilippinesMaria Mikaela MarcelinoPas encore d'évaluation
- Whole Brain Lesson Plan: 3 QuarterDocument5 pagesWhole Brain Lesson Plan: 3 QuarterNieve Marie Cerezo100% (1)
- Volleyball ReflectionDocument1 pageVolleyball ReflectionJake Santos100% (1)
- Hamodia Parsonage ArticleDocument2 pagesHamodia Parsonage ArticleJudah KupferPas encore d'évaluation
- Lincoln's Last Trial by Dan AbramsDocument6 pagesLincoln's Last Trial by Dan AbramsdosatoliPas encore d'évaluation
- Firewalker Spell and Ability GuideDocument2 pagesFirewalker Spell and Ability GuideRon Van 't VeerPas encore d'évaluation
- Shell Rimula R7 AD 5W-30: Performance, Features & Benefits Main ApplicationsDocument2 pagesShell Rimula R7 AD 5W-30: Performance, Features & Benefits Main ApplicationsAji WibowoPas encore d'évaluation
- Gautam KDocument12 pagesGautam Kgautam kayapakPas encore d'évaluation
- QuizInfo8 6 10Document373 pagesQuizInfo8 6 10Gill BeroberoPas encore d'évaluation
- Deep Work Book - English ResumoDocument9 pagesDeep Work Book - English ResumoJoão Pedro OnozatoPas encore d'évaluation
- ECUMINISMDocument2 pagesECUMINISMarniel somilPas encore d'évaluation
- Artificial IntelligenceDocument1 pageArtificial IntelligenceTeresaPas encore d'évaluation
- Java Thread Priority in MultithreadingDocument3 pagesJava Thread Priority in MultithreadingMITALI SHARMAPas encore d'évaluation
- Free ArtistDocument1 pageFree Artistnunomgalmeida-1Pas encore d'évaluation
- Eng CBLDocument2 pagesEng CBLMengTangPas encore d'évaluation
- Smart Irrigation System With Lora & Recording of Lora Broadcast Using RTL-SDR Dongle For Spectrum AnalyzationDocument4 pagesSmart Irrigation System With Lora & Recording of Lora Broadcast Using RTL-SDR Dongle For Spectrum AnalyzationInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- AR118 - MSDS 2023 (Chemlube) - 19.10.2023Document8 pagesAR118 - MSDS 2023 (Chemlube) - 19.10.2023sanichi135Pas encore d'évaluation
- Noise Pollution Control Policy IndiaDocument10 pagesNoise Pollution Control Policy IndiaAllu GiriPas encore d'évaluation
- Inmarsat M2M Terminal ComparisonDocument2 pagesInmarsat M2M Terminal Comparisonmaruka33Pas encore d'évaluation
- Additional Practice Questions on Bonding and Mechanical Properties of MaterialsDocument26 pagesAdditional Practice Questions on Bonding and Mechanical Properties of MaterialsYeo JosephPas encore d'évaluation
- Smoochie Monsterpants: I Have Added My Pattern To RavelryDocument3 pagesSmoochie Monsterpants: I Have Added My Pattern To RavelryadinaPas encore d'évaluation
- Pines City Colleges: College of NursingDocument2 pagesPines City Colleges: College of NursingmagisasamundoPas encore d'évaluation
- Shah Wali Ullah Syed Haji Shariat Ullah Ahmad Barelvi (Notes)Document2 pagesShah Wali Ullah Syed Haji Shariat Ullah Ahmad Barelvi (Notes)Samreen KapasiPas encore d'évaluation
- Remotely Operated Underwater Vehicle With 6DOF Robotic ArmDocument14 pagesRemotely Operated Underwater Vehicle With 6DOF Robotic ArmMethun RajPas encore d'évaluation
- Income Tax BotswanaDocument15 pagesIncome Tax BotswanaFrancisPas encore d'évaluation
- Ce QuizDocument2 pagesCe QuizCidro Jake TyronPas encore d'évaluation
- 100 Inspirational Quotes On LearningDocument9 pages100 Inspirational Quotes On LearningGlenn VillegasPas encore d'évaluation