Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Name: Insong, Osannah Irish B.: No, There IsDocument1 pageName: Insong, Osannah Irish B.: No, There IsOsannah Irish InsongPas encore d'évaluation
- WUNSCH A - Skin Eye and BrainDocument4 pagesWUNSCH A - Skin Eye and BrainAlexander WunschPas encore d'évaluation
- Cushing's Disease: A New Approach To Therapy in Equine and Canine PatientsDocument4 pagesCushing's Disease: A New Approach To Therapy in Equine and Canine PatientsYumeChanPas encore d'évaluation
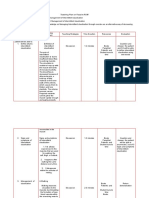
- Teaching Plan MeeeeeDocument6 pagesTeaching Plan MeeeeeJenyl BajadoPas encore d'évaluation
- Dosage & Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Rivotril ClassificationDocument5 pagesDosage & Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Rivotril ClassificationJenyl BajadoPas encore d'évaluation
- A Case Study of Urinary Tract Infection 2Document23 pagesA Case Study of Urinary Tract Infection 2Jenyl BajadoPas encore d'évaluation
- Drug Dosage Action/Indication Side Effect Contraindications Nursing Responsibility AmpicillinDocument1 pageDrug Dosage Action/Indication Side Effect Contraindications Nursing Responsibility AmpicillinJenyl BajadoPas encore d'évaluation
- Application of Demographic Transition On Health Program PlanningDocument5 pagesApplication of Demographic Transition On Health Program PlanningJenyl BajadoPas encore d'évaluation
- Life-Cycle of Entamoeba HistolyticaDocument15 pagesLife-Cycle of Entamoeba HistolyticaJenyl BajadoPas encore d'évaluation
- Nutrition During Childhood and AdolescentDocument40 pagesNutrition During Childhood and AdolescentJenyl BajadoPas encore d'évaluation
- LactationDocument24 pagesLactationJenyl Bajado100% (1)
- 2nd Pediatric Endocrinology CME FinalDocument2 pages2nd Pediatric Endocrinology CME FinaldrnamithapedPas encore d'évaluation
- Hypothyroidism Concept MapDocument1 pageHypothyroidism Concept Mapel shilohPas encore d'évaluation
- Ata Hyperthyroidism BrochureDocument3 pagesAta Hyperthyroidism BrochureKumalaAudiKusumaPas encore d'évaluation
- Excretory NotesDocument8 pagesExcretory NotesJasminePas encore d'évaluation
- Methods of ContraceptionDocument24 pagesMethods of ContraceptionAnonymous XLMsbQqPas encore d'évaluation
- B1 Nerves Hormones Homeostasis HigherDocument15 pagesB1 Nerves Hormones Homeostasis HigherdownendsciencePas encore d'évaluation
- Studii Clinice Active 2021 Prof. BadiuDocument1 pageStudii Clinice Active 2021 Prof. BadiucypykPas encore d'évaluation
- Neoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerDocument57 pagesNeoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerNavya SreePas encore d'évaluation
- Hioerplasia Mamaria GestacionalDocument9 pagesHioerplasia Mamaria GestacionalOctavio LeyvaPas encore d'évaluation
- IVFDocument168 pagesIVFAbhishek Vijayakumar100% (3)
- Q. What Is The Difference Between Myxedema and Hypothyroidism?Document4 pagesQ. What Is The Difference Between Myxedema and Hypothyroidism?Wan Razin Wan HassanPas encore d'évaluation
- Prevalence of Hypothyroidism in Adults An EpidemioDocument6 pagesPrevalence of Hypothyroidism in Adults An EpidemioCindy Auliah NasutionPas encore d'évaluation
- SkinDocument20 pagesSkinDr. Mary MjeedPas encore d'évaluation
- Project Ease Biology Module 13Document30 pagesProject Ease Biology Module 13Kebb Patrick Enar75% (4)
- Hypothyroidism in AyurvedaDocument35 pagesHypothyroidism in Ayurvedagarry_pooja100% (4)
- Pharma Rapid Review FOCUSDocument85 pagesPharma Rapid Review FOCUSKeelPas encore d'évaluation
- Pharmacotherapy - Thyroid Disorder PDFDocument63 pagesPharmacotherapy - Thyroid Disorder PDFnadiah100% (3)
- Fragile X Associated Primary Ovarian Insufficiency (FXPOI) : Case Report and Literature ReviewDocument12 pagesFragile X Associated Primary Ovarian Insufficiency (FXPOI) : Case Report and Literature Review6 APas encore d'évaluation
- New Estrogen and ProgesteroneDocument56 pagesNew Estrogen and ProgesteroneHBrPas encore d'évaluation
- Bio 473 Reproductive Endocrinology Lab Compiled LabDocument10 pagesBio 473 Reproductive Endocrinology Lab Compiled Labapi-253602935Pas encore d'évaluation
- The Integumentary System Has Multiple Roles in HomeostasisDocument3 pagesThe Integumentary System Has Multiple Roles in HomeostasisRj CorderoPas encore d'évaluation
- Menstrual CycleDocument6 pagesMenstrual CycleKyndra Maxynne CamachoPas encore d'évaluation
- A Suggested Protocol For The Endocrine Postoperative Management of Patients Undergoing Pituitary SurgeryDocument11 pagesA Suggested Protocol For The Endocrine Postoperative Management of Patients Undergoing Pituitary Surgerymiguel saba sabaPas encore d'évaluation
- PT - Araling Panlipunan 4 - Q2Document2 pagesPT - Araling Panlipunan 4 - Q2MARVIN CARMELOPas encore d'évaluation
- Ovarian Cyst Treatment 1Document5 pagesOvarian Cyst Treatment 1Helcio FerreiraPas encore d'évaluation
- Etiology of Breast CarcinomaDocument11 pagesEtiology of Breast Carcinomashrutik91Pas encore d'évaluation
- Final Exam Phys2130 SU15 Version 1 - Answer KeyDocument17 pagesFinal Exam Phys2130 SU15 Version 1 - Answer KeycoolsuernamePas encore d'évaluation