Vous aimerez peut-être aussi
- S 104 LBLDocument15 pagesS 104 LBLEko YuliantoPas encore d'évaluation
- Brufen Sustained Release (SR) : Data SheetDocument11 pagesBrufen Sustained Release (SR) : Data SheetPrince Ali100% (1)
- IBUPROFEN (Arrowcare) : PresentationDocument6 pagesIBUPROFEN (Arrowcare) : PresentationShirmayne TangPas encore d'évaluation
- Ibuprofen Arrow Care TabDocument9 pagesIbuprofen Arrow Care TabshajahanputhusseriPas encore d'évaluation
- New Zealand Data Sheet Ibuprofen 1. Product Name: 4.1 Therapeutic IndicationsDocument15 pagesNew Zealand Data Sheet Ibuprofen 1. Product Name: 4.1 Therapeutic IndicationsGpromotsPas encore d'évaluation
- Brufen: New Zealand Data SheetDocument12 pagesBrufen: New Zealand Data SheetFsPas encore d'évaluation
- Pi Ibugesic Fever and PainDocument20 pagesPi Ibugesic Fever and PainAndrew PartridgePas encore d'évaluation
- Summary of Product Characteristics: Apsifen-F Ibuprofen 600 MG Film-Coated TabletsDocument12 pagesSummary of Product Characteristics: Apsifen-F Ibuprofen 600 MG Film-Coated TabletsMeriam Gita Maulia SuhaidiPas encore d'évaluation
- Etoricoxib 120 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)Document1 pageEtoricoxib 120 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)vikasjha12345Pas encore d'évaluation
- Ibuprofen 150mg + Paracetamol 500mg (Combodex)Document15 pagesIbuprofen 150mg + Paracetamol 500mg (Combodex)ddandan_2Pas encore d'évaluation
- SE Brufen 2% SMPCDocument13 pagesSE Brufen 2% SMPCSrechko MilichPas encore d'évaluation
- Core Safety ProfileDocument7 pagesCore Safety Profileblue diamondPas encore d'évaluation
- SE - Brufen 800 - SMPCDocument12 pagesSE - Brufen 800 - SMPCSrechko MilichPas encore d'évaluation
- Physician's Prescribing Information Etopan 200and 300 MG Capsules Etopan 400 and 500 MG TabletsDocument11 pagesPhysician's Prescribing Information Etopan 200and 300 MG Capsules Etopan 400 and 500 MG Tabletsddandan_2Pas encore d'évaluation
- Ketorolac Tromethamine Injection Usp: Product MonographDocument41 pagesKetorolac Tromethamine Injection Usp: Product MonographWahyu AriawanPas encore d'évaluation
- Angeliq PM enDocument45 pagesAngeliq PM enTomacho HitachiPas encore d'évaluation
- BPS 2143 PharmacologyDocument15 pagesBPS 2143 PharmacologyBella AstilahPas encore d'évaluation
- Prescribing Information Abiratred Abiraterone Acetate Tablets 250 MGDocument9 pagesPrescribing Information Abiratred Abiraterone Acetate Tablets 250 MGChrisPas encore d'évaluation
- Etoricoxib DS MSD2017Document27 pagesEtoricoxib DS MSD2017Anderson T BPas encore d'évaluation
- Acetylcysteine 200mg (Siran, Reolin)Document5 pagesAcetylcysteine 200mg (Siran, Reolin)ddandan_2Pas encore d'évaluation
- SE - Brufen 200400600 - SMPCDocument13 pagesSE - Brufen 200400600 - SMPCSrechko MilichPas encore d'évaluation
- Analgesic: Mefenamic AcidDocument5 pagesAnalgesic: Mefenamic Acidmegazhang94Pas encore d'évaluation
- Primolut N en PiDocument7 pagesPrimolut N en PiXamanPas encore d'évaluation
- Cytotec® Misoprostol TabletsDocument12 pagesCytotec® Misoprostol Tabletssuhandi71Pas encore d'évaluation
- Warfarin - Drug InformationDocument23 pagesWarfarin - Drug InformationTestestePas encore d'évaluation
- Name of The Medicinal Product: AdultsDocument9 pagesName of The Medicinal Product: Adultsddandan_2Pas encore d'évaluation
- Oxytocin Generic Name: Oxytocin Brand Name: Pitocin/ Syntocinon IndicationsDocument5 pagesOxytocin Generic Name: Oxytocin Brand Name: Pitocin/ Syntocinon IndicationsKish SuguitanPas encore d'évaluation
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakPas encore d'évaluation
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakPas encore d'évaluation
- New Zealand Data Sheet Nurofen Plus: 1. Trade Name of The Medicinal ProductDocument15 pagesNew Zealand Data Sheet Nurofen Plus: 1. Trade Name of The Medicinal ProductPhilipPas encore d'évaluation
- VBBVBVBVBVBVBVBBVDocument17 pagesVBBVBVBVBVBVBVBBVAYUE ZONE PRATITISPas encore d'évaluation
- Pyridostigmine BromideDocument4 pagesPyridostigmine BromideRavinderenPichan100% (1)
- The Use of Proton Pump Inhibitors in Treating and Preventing NSAID-induced Mucosal DamageDocument6 pagesThe Use of Proton Pump Inhibitors in Treating and Preventing NSAID-induced Mucosal DamageFriska Rachmanita PrayogoPas encore d'évaluation
- Name Mucosta Tablets 100 Description PDFDocument7 pagesName Mucosta Tablets 100 Description PDFnanda RaharjaPas encore d'évaluation
- MisoprostolDocument11 pagesMisoprostolMaulidya FakhrulPas encore d'évaluation
- April 2019-0Document25 pagesApril 2019-0SEIYADU IBRAHIM KPas encore d'évaluation
- SUMMARY OF PRODUCT CHARACTERISTICS Ibuprofen and Codeine 200mg/12.8mg Film-Coated TabletsDocument12 pagesSUMMARY OF PRODUCT CHARACTERISTICS Ibuprofen and Codeine 200mg/12.8mg Film-Coated TabletsDane WoodPas encore d'évaluation
- SMPC UKDocument15 pagesSMPC UKSrechko MilichPas encore d'évaluation
- Azathioprine PDFDocument3 pagesAzathioprine PDFAnca AnkaPas encore d'évaluation
- AnalgetikDocument58 pagesAnalgetiksaraswaty710Pas encore d'évaluation
- Drug Presentation AtropineDocument6 pagesDrug Presentation AtropineShivam Malik100% (1)
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument15 pagesSummary of Product Characteristics: 4.1 Therapeutic Indicationsdilka dariyaPas encore d'évaluation
- Apremilast PI Europe Aug 2019Document14 pagesApremilast PI Europe Aug 2019Wei Sheng ChongPas encore d'évaluation
- Augmentin I VDocument14 pagesAugmentin I VShankar JothiPas encore d'évaluation
- Azimor - 250 TabletsDocument1 pageAzimor - 250 TabletsRakesh PalPas encore d'évaluation
- Drugs Study Pedia PDFDocument8 pagesDrugs Study Pedia PDFmark angeloPas encore d'évaluation
- Ecotrin (ASA 81mg)Document3 pagesEcotrin (ASA 81mg)E100% (1)
- Anx 130395 enDocument48 pagesAnx 130395 enMehdiPas encore d'évaluation
- AzathioprineDocument3 pagesAzathioprinesky.bluePas encore d'évaluation
- AzathioprineDocument14 pagesAzathioprineNur Wakhid HidayatPas encore d'évaluation
- Ibuprofen - A Journey From Prescription To Over-The-counterDocument5 pagesIbuprofen - A Journey From Prescription To Over-The-counterPharmazellPas encore d'évaluation
- New Zealand Data Sheet: Primolut N® Qualitative and Quantitative CompositionDocument13 pagesNew Zealand Data Sheet: Primolut N® Qualitative and Quantitative CompositionMohammed ShakilPas encore d'évaluation
- MisopaDocument2 pagesMisopaSaifur Rahman SuzonPas encore d'évaluation
- 018332s032lbl PDFDocument34 pages018332s032lbl PDFAshraf OtroshPas encore d'évaluation
- uk-spc-nexium-DRESS-update-GI 21 0009aDocument17 pagesuk-spc-nexium-DRESS-update-GI 21 0009aDeisy ClerkePas encore d'évaluation
- Lipid DisorderDocument5 pagesLipid DisorderZahida BashirPas encore d'évaluation
- FebuxostatDocument14 pagesFebuxostatSanjay NavalePas encore d'évaluation
- Drug StudiesDocument16 pagesDrug Studiesvitcloud23100% (2)
- Esomeprazole Tablets GranulesDocument57 pagesEsomeprazole Tablets GranulesMohammed shamiul ShahidPas encore d'évaluation
- Lipid Lowering Agents IDocument14 pagesLipid Lowering Agents IRALPH ELVIN MACANLALAYPas encore d'évaluation
- Cholinergic AgonistsDocument25 pagesCholinergic AgonistsRahul VadlapatlaPas encore d'évaluation
- Tramadol Drug-StudyDocument3 pagesTramadol Drug-StudyPang ProjectPas encore d'évaluation
- Bola CommunityDocument5 pagesBola CommunityOladimeji Raphael OnibonPas encore d'évaluation
- EE MOCK Test 2 Jan 2017 Questions OnlyDocument28 pagesEE MOCK Test 2 Jan 2017 Questions OnlyEmadSamirPas encore d'évaluation
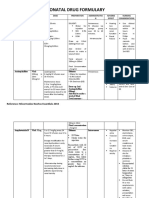
- Neonatal Drug FormularyDocument6 pagesNeonatal Drug FormularyLucian CaelumPas encore d'évaluation
- Mehrotra Family Clinic: Vaccination: MedicineDocument1 pageMehrotra Family Clinic: Vaccination: MedicineManohar KaurPas encore d'évaluation
- Hospital Training ReportDocument19 pagesHospital Training ReportRitik Thakur67% (24)
- Membership Statewise PDFDocument16 pagesMembership Statewise PDFKartik TurakhiaPas encore d'évaluation
- Pharmacology MCQs 2Document6 pagesPharmacology MCQs 2Waseem SarwarPas encore d'évaluation
- Rationaldruguse 150519185142 Lva1 App6892Document12 pagesRationaldruguse 150519185142 Lva1 App6892nikki_bamsPas encore d'évaluation
- Nasal Drug Delivery SystemDocument46 pagesNasal Drug Delivery Systemrat001100% (1)
- Chapter 5 Antifungal DrugsDocument55 pagesChapter 5 Antifungal DrugsAssssssPas encore d'évaluation
- Pharmacology: Animation 18.1: 3D-Animation Source & Credit: Rikkyo - AcDocument14 pagesPharmacology: Animation 18.1: 3D-Animation Source & Credit: Rikkyo - AcWorld of FunPas encore d'évaluation
- PHARM 315: Cheza May Baldado BS Pharm IIIDocument12 pagesPHARM 315: Cheza May Baldado BS Pharm IIIKathleen B BaldadoPas encore d'évaluation
- 1-Generic Name 2-Trade Name: LIPITOR:: AtorvastatinDocument11 pages1-Generic Name 2-Trade Name: LIPITOR:: AtorvastatinNouran BakrPas encore d'évaluation
- Part 1 Pharm ModuleDocument49 pagesPart 1 Pharm ModuleJojo JustoPas encore d'évaluation
- Librium ChlordiazepoxideDocument2 pagesLibrium ChlordiazepoxideEPas encore d'évaluation
- Deal AMA PABRIK 02.05.2023Document26 pagesDeal AMA PABRIK 02.05.2023Afif SetiawanPas encore d'évaluation
- GDHHDocument40 pagesGDHHnaelarizqiPas encore d'évaluation
- 100 Dosage Calculation Practice Problems AnswersDocument12 pages100 Dosage Calculation Practice Problems AnswersTeena Real81% (21)
- Jurnal Data Puslitdatin BNN 2018 - ENDocument240 pagesJurnal Data Puslitdatin BNN 2018 - ENAnti NarkobaPas encore d'évaluation
- OTC Drug ListDocument7 pagesOTC Drug ListHong Diem100% (1)
- Pharmacology Concept BookDocument357 pagesPharmacology Concept Bookram dheerPas encore d'évaluation
- Bioactive Compounds in PlantsDocument32 pagesBioactive Compounds in PlantsTilahun BelaynehPas encore d'évaluation
- ImmunizationDocument40 pagesImmunizationHilyaJae-heePas encore d'évaluation
- Dosage Calculations (Adult and Pediatrics)Document7 pagesDosage Calculations (Adult and Pediatrics)kirsleone_16293757Pas encore d'évaluation
- Supply Chain Solutions For RanbaxyDocument10 pagesSupply Chain Solutions For RanbaxyMesajalPas encore d'évaluation
- Dispinsing Activity by GroupDocument2 pagesDispinsing Activity by Groupsybyl formenteraPas encore d'évaluation
- Pharmaceutical Formulations III Pharm DQuestion BankDocument7 pagesPharmaceutical Formulations III Pharm DQuestion BankAnanda VijayasarathyPas encore d'évaluation