Vous aimerez peut-être aussi
- Planning Rural Hospital Emerging Infectious Disease ExercisesDocument32 pagesPlanning Rural Hospital Emerging Infectious Disease ExercisesParyanto Hippii SoloPas encore d'évaluation
- Infectious 1Document29 pagesInfectious 1ericamaedgPas encore d'évaluation
- Environmental cleaning and disinfection: Principles of infection transmission and the role of the environmentDocument53 pagesEnvironmental cleaning and disinfection: Principles of infection transmission and the role of the environmentIsaacPas encore d'évaluation
- Obg Ward Teaching Infection ControlDocument37 pagesObg Ward Teaching Infection ControlbhavanaPas encore d'évaluation
- Journal of Biomedical and Pharmaceutical Research: ISSN (Online) : 2279-0594 ISSN (Print) : 2589-8752Document4 pagesJournal of Biomedical and Pharmaceutical Research: ISSN (Online) : 2279-0594 ISSN (Print) : 2589-8752Alexandru Codrin-IonutPas encore d'évaluation
- Patient Safety and Biohazard SafetyDocument40 pagesPatient Safety and Biohazard Safetyniharikaa1230Pas encore d'évaluation
- Env Surface DisDocument18 pagesEnv Surface DisSabeen KhurshidPas encore d'évaluation
- Basic Infection Control Skills License (BICSL) Quick ReviewerDocument13 pagesBasic Infection Control Skills License (BICSL) Quick Reviewerمحمد ابراهيمPas encore d'évaluation
- Indicators, Disinfection and Sterilization SG 092019Document11 pagesIndicators, Disinfection and Sterilization SG 092019Meena CtPas encore d'évaluation
- Infectioncontrolprevention 230411093422 62e04757Document42 pagesInfectioncontrolprevention 230411093422 62e04757bahjaa445Pas encore d'évaluation
- Disinfection Policy Jipmer 2019Document32 pagesDisinfection Policy Jipmer 2019ishitaabhandari1968Pas encore d'évaluation
- DISINFECTION GUIDELINES 2nd EDITION 2019Document42 pagesDISINFECTION GUIDELINES 2nd EDITION 2019miziezuraPas encore d'évaluation
- Dental Clinics DesinfeccionDocument23 pagesDental Clinics DesinfeccionOrtodoncia UNAL 2020Pas encore d'évaluation
- B. Surgical ManagementDocument20 pagesB. Surgical ManagementNickaela CalalangPas encore d'évaluation
- Lesson Notes HWDocument16 pagesLesson Notes HWNlida LieydaPas encore d'évaluation
- Nightingale Student Guide - Medical AsepsisDocument8 pagesNightingale Student Guide - Medical Asepsismanmeetboparai146Pas encore d'évaluation
- Infrastructure Requirements for Quality HIV ServicesDocument36 pagesInfrastructure Requirements for Quality HIV ServicesJedan TopiagonPas encore d'évaluation
- European Infectious Disease: Volume 6 - Issue 2 - Winter 2012 - ExtractDocument7 pagesEuropean Infectious Disease: Volume 6 - Issue 2 - Winter 2012 - Extractkasu s reddyPas encore d'évaluation
- Formulation and Evaluation of Herbal Sanitizer PDFDocument4 pagesFormulation and Evaluation of Herbal Sanitizer PDFWikoo EPas encore d'évaluation
- Health Care Workers' Hand Contamination Levels and Antibacterial EfficacyDocument4 pagesHealth Care Workers' Hand Contamination Levels and Antibacterial EfficacyHùng Nguyễn ViệtPas encore d'évaluation
- Potential Nursing Diagnosis: Risk for InfectionDocument2 pagesPotential Nursing Diagnosis: Risk for InfectionKarl KiwisPas encore d'évaluation
- Infection Control 2Document83 pagesInfection Control 2mrbyy619Pas encore d'évaluation
- Screenshot 2020-12-13 at 3.47.43 PM PDFDocument45 pagesScreenshot 2020-12-13 at 3.47.43 PM PDFJihad HassanPas encore d'évaluation
- Environmental CleaningDocument55 pagesEnvironmental Cleaningriffat shaheenPas encore d'évaluation
- Materi Hand HygieneDocument35 pagesMateri Hand HygieneDwi AstutiPas encore d'évaluation
- PHINMA University Nursing AssessmentDocument2 pagesPHINMA University Nursing AssessmentVoid LessPas encore d'évaluation
- Lesson 1 - Microbial ControlDocument3 pagesLesson 1 - Microbial ControlA CPas encore d'évaluation
- Surface Disinfection: Choosing The Right DisinfectantDocument3 pagesSurface Disinfection: Choosing The Right DisinfectantSanti utamiPas encore d'évaluation
- The Ideal disinfectant-GPS-0620Document5 pagesThe Ideal disinfectant-GPS-0620sumiya mashadiPas encore d'évaluation
- ICU infection controlDocument37 pagesICU infection controlVidit JoshiPas encore d'évaluation
- Healthcare-Associated Infections Prevention LessonDocument13 pagesHealthcare-Associated Infections Prevention Lessonvanessa balatucanPas encore d'évaluation
- Rev. sci. tech. Off. int. Epiz., 1995,14 (1), 105-122Document18 pagesRev. sci. tech. Off. int. Epiz., 1995,14 (1), 105-122RENZO ISAIAS SANTILLAN ZEVALLOSPas encore d'évaluation
- Managing Biomedical Waste in HospitalsDocument15 pagesManaging Biomedical Waste in Hospitalskathyayani arraPas encore d'évaluation
- Management of Outbreak in NICU - Lily RundjanDocument43 pagesManagement of Outbreak in NICU - Lily RundjanBayu KurniawanPas encore d'évaluation
- Infection Control in The CSSD Unit: Micah Lettsome, CSSD Technician Tuesday 28 September, 2021Document10 pagesInfection Control in The CSSD Unit: Micah Lettsome, CSSD Technician Tuesday 28 September, 2021Micah LettsomePas encore d'évaluation
- Teknik Aseptik SaatPraktikumKedokteran GigiDocument26 pagesTeknik Aseptik SaatPraktikumKedokteran Gigizurafs dhanysPas encore d'évaluation
- Environmental Hygiene - The Importance of Process, Product and Practice PDFDocument18 pagesEnvironmental Hygiene - The Importance of Process, Product and Practice PDFAnsh KunalPas encore d'évaluation
- SCP Infection ControlDocument7 pagesSCP Infection ControlNoreen PunjwaniPas encore d'évaluation
- Infection Precaution, HTMDocument32 pagesInfection Precaution, HTMAuzaniAkraminAhmadPas encore d'évaluation
- Effektifitas Larutan AlkoholDocument6 pagesEffektifitas Larutan AlkoholpicobodasPas encore d'évaluation
- Infection ControlDocument29 pagesInfection Controlkishoremanisha87Pas encore d'évaluation
- M10 FundaDocument6 pagesM10 FundaAl-Khan HadjailPas encore d'évaluation
- BNC06255 Ihs300cpd CW01Document15 pagesBNC06255 Ihs300cpd CW01thilinaPas encore d'évaluation
- The Chain of Infection What Is An Infection?: Peel Public Health - Take Control Guide 2013Document5 pagesThe Chain of Infection What Is An Infection?: Peel Public Health - Take Control Guide 2013Kamran KhanPas encore d'évaluation
- Tracheostomy Care Lesson PlanDocument26 pagesTracheostomy Care Lesson PlanShubha JeniferPas encore d'évaluation
- Cleaning, Disinfection, and Sterilization of Medical EquipmentDocument31 pagesCleaning, Disinfection, and Sterilization of Medical EquipmentameliariskyPas encore d'évaluation
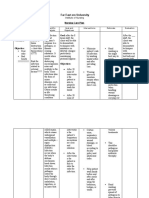
- Far East Ern University: Nursing Care PlanDocument6 pagesFar East Ern University: Nursing Care PlanmharieeePas encore d'évaluation
- Kozier FundamentalDocument50 pagesKozier FundamentalgkixPas encore d'évaluation
- Original Article - Pharmaceutical Research Evaluation of Fungicidal Activity of Herbal Hand SanitizerDocument5 pagesOriginal Article - Pharmaceutical Research Evaluation of Fungicidal Activity of Herbal Hand SanitizerIqbal PutraPas encore d'évaluation
- Chapter 12Document35 pagesChapter 12BRENDHIL PACIFICO CRUZPas encore d'évaluation
- Fundamental Aspects of Infection Prevention and ControlD'EverandFundamental Aspects of Infection Prevention and ControlPas encore d'évaluation
- Efficacy of hospital disinfectants against pathogensDocument10 pagesEfficacy of hospital disinfectants against pathogensMariaPas encore d'évaluation
- Antisepsis/Disinfection/Sterilization: S4 Oral Abstracts / American Journal of Infection Control 47 (2019) S2 S14Document1 pageAntisepsis/Disinfection/Sterilization: S4 Oral Abstracts / American Journal of Infection Control 47 (2019) S2 S14Khansa LuthfiyyahPas encore d'évaluation
- Brochure 1Document2 pagesBrochure 1aoife0412Pas encore d'évaluation
- PCDS NCP Surgery Ward DSPHDocument2 pagesPCDS NCP Surgery Ward DSPHJhomines NialaPas encore d'évaluation
- American Journal of Infection Control: Reviews & CommentsDocument8 pagesAmerican Journal of Infection Control: Reviews & CommentsCatalin DucuPas encore d'évaluation
- Dr. Md. Mujibur Rahman: Ahsanullah University of Science & Technology (AUST)Document18 pagesDr. Md. Mujibur Rahman: Ahsanullah University of Science & Technology (AUST)Mohaiminur ArponPas encore d'évaluation
- Control of Hospital Acquired Infection PDFDocument36 pagesControl of Hospital Acquired Infection PDFPrakashPas encore d'évaluation
- Guidelines For Cleaning Disinfection and Sterilisation of Patient Care Equipment Staff ResponsibilitiesDocument28 pagesGuidelines For Cleaning Disinfection and Sterilisation of Patient Care Equipment Staff ResponsibilitiesbiomedmaulikPas encore d'évaluation
- WHAT NOT TO DO AFTER PEST CONTROL SPRAYSD'EverandWHAT NOT TO DO AFTER PEST CONTROL SPRAYSPas encore d'évaluation
- Kidney 4.1.0.0.rel CapcpDocument18 pagesKidney 4.1.0.0.rel CapcpkarimahihdaPas encore d'évaluation
- Mitochondrial Cytopathies in Children and AdultsDocument28 pagesMitochondrial Cytopathies in Children and AdultsmmaitehmdPas encore d'évaluation
- Blue Legs - A New Long-COVID Symptom How To Test For and Treat It - Docx #@Document27 pagesBlue Legs - A New Long-COVID Symptom How To Test For and Treat It - Docx #@Dan TudorPas encore d'évaluation
- Border Terrier Ukc StandardDocument2 pagesBorder Terrier Ukc Standardapi-342444556Pas encore d'évaluation
- Psychosis ObjectivesDocument14 pagesPsychosis ObjectivesfatenPas encore d'évaluation
- GEHC Brochure Senographe CareDocument7 pagesGEHC Brochure Senographe CareVremedSoluCionesPas encore d'évaluation
- Cement CSRDocument35 pagesCement CSRKasak Gupta100% (1)
- Chapter 7 Africa South of The SaharaDocument40 pagesChapter 7 Africa South of The Saharafuck ypouPas encore d'évaluation
- Cannabis Use and Disorder - Epidemiology, Comorbidity, Health Consequences, and Medico-Legal Status - UpToDateDocument34 pagesCannabis Use and Disorder - Epidemiology, Comorbidity, Health Consequences, and Medico-Legal Status - UpToDateAnonymous kvI7zBNPas encore d'évaluation
- Kirit P. Mehta School of Law, Mumbai: A Project Submitted ONDocument12 pagesKirit P. Mehta School of Law, Mumbai: A Project Submitted ONNikit BaryaPas encore d'évaluation
- Neuromuscular Therapy Techniques for Stroke and MS RehabilitationDocument11 pagesNeuromuscular Therapy Techniques for Stroke and MS RehabilitationWenzy Razzie cruzPas encore d'évaluation
- AABB Billing Guide For Blood Products and Related Services: July 2020 1Document45 pagesAABB Billing Guide For Blood Products and Related Services: July 2020 1Rija KhanPas encore d'évaluation
- NEET Biology Through MCQDocument587 pagesNEET Biology Through MCQAnanth Dharanidharan100% (1)
- 5388 Tech ManualDocument198 pages5388 Tech ManualMichal SzymanskiPas encore d'évaluation
- Vicente vs. Employees' Compensation CommissionDocument7 pagesVicente vs. Employees' Compensation CommissionAlexPas encore d'évaluation
- Non-Profit Organization Funds Gregory Grabovoi TeachingsDocument95 pagesNon-Profit Organization Funds Gregory Grabovoi Teachingsssss87va93% (27)
- WORKSHEET 3 Lymphocyte ActivationDocument5 pagesWORKSHEET 3 Lymphocyte ActivationNeha ChoudharyPas encore d'évaluation
- Anti-Rabies Act of 2007 (Ra 9482) 2Document29 pagesAnti-Rabies Act of 2007 (Ra 9482) 2Ronz Rogan100% (1)
- Family Case Study For HydrocephalusDocument9 pagesFamily Case Study For HydrocephalusjaegergranPas encore d'évaluation
- Basic Life Support Field GuideDocument56 pagesBasic Life Support Field GuidelmaoheartsPas encore d'évaluation
- Pediatrics ImpDocument233 pagesPediatrics Impملك عيسى100% (1)
- 4446 16364 1 PBDocument8 pages4446 16364 1 PBSafira Rosyadatul AissyPas encore d'évaluation
- Food PreparationDocument127 pagesFood PreparationRUMBIDZAI MELLISA DZINZIPas encore d'évaluation
- Inspiration Powerpoint NoteDocument13 pagesInspiration Powerpoint Noteapi-201676767Pas encore d'évaluation
- Human Cannibalism 1Document8 pagesHuman Cannibalism 1api-409100981Pas encore d'évaluation
- Transfusion-Related Acute Lung Injury: HistoryDocument20 pagesTransfusion-Related Acute Lung Injury: HistoryBladimir CentenoPas encore d'évaluation
- Kim (2015) - Lemon Detox Diet Reduced Body FatDocument12 pagesKim (2015) - Lemon Detox Diet Reduced Body FatRodrigo MelloPas encore d'évaluation
- Daftar PustakaDocument3 pagesDaftar PustakaAlmira PutriPas encore d'évaluation
- Physical Education Mcqs For All Govt ExamDocument108 pagesPhysical Education Mcqs For All Govt Examrabiaghafar855Pas encore d'évaluation
- Venipuncture Techniques and ProceduresDocument66 pagesVenipuncture Techniques and ProceduresAngelica Camille B. AbaoPas encore d'évaluation