Vous aimerez peut-être aussi
- Analog CommunicationDocument110 pagesAnalog CommunicationSyed AshmadPas encore d'évaluation
- Verilog Language: Lexical Conventions ExamplesDocument4 pagesVerilog Language: Lexical Conventions Examplesvenkata charyPas encore d'évaluation
- WWW - Manaresults.co - In: Applications (Common To ECE, ETM)Document2 pagesWWW - Manaresults.co - In: Applications (Common To ECE, ETM)Syed AshmadPas encore d'évaluation
- DDVLECE 2 Marks QuestionsDocument6 pagesDDVLECE 2 Marks QuestionsSyed AshmadPas encore d'évaluation
- Femur Bone Volumetric Estimation From A Single2006Document4 pagesFemur Bone Volumetric Estimation From A Single2006Syed AshmadPas encore d'évaluation
- Jntu Hyderabad - B.tech - Linear and Digital Ic Applications r13 115eb032017 FR 81Document2 pagesJntu Hyderabad - B.tech - Linear and Digital Ic Applications r13 115eb032017 FR 81Syed AshmadPas encore d'évaluation
- RT 31026042019Document1 pageRT 31026042019Syed AshmadPas encore d'évaluation
- 01 MI IntroductionDocument72 pages01 MI IntroductionRicardo BaptistaPas encore d'évaluation
- Digital Design Through Verilog HDL Course Outcomes For LabDocument1 pageDigital Design Through Verilog HDL Course Outcomes For LabSyed AshmadPas encore d'évaluation
- X RayDocument18 pagesX RaySyed AshmadPas encore d'évaluation
- Texture Analysis and Fracture IdentificatDocument5 pagesTexture Analysis and Fracture IdentificatSyed AshmadPas encore d'évaluation
- An Image Processing Algorithm To Estimate Bone2017Document4 pagesAn Image Processing Algorithm To Estimate Bone2017Syed AshmadPas encore d'évaluation
- DDVLECE 2 Marks QuestionsDocument6 pagesDDVLECE 2 Marks QuestionsSyed AshmadPas encore d'évaluation
- JNTU Anantapur B.Tech Exam Results December 2014Document184 pagesJNTU Anantapur B.Tech Exam Results December 2014Syed AshmadPas encore d'évaluation
- Bone Mineral Density and Bone Mineral Content2007Document4 pagesBone Mineral Density and Bone Mineral Content2007Syed AshmadPas encore d'évaluation
- Digital Image Processing and Soft Computing TechniquesDocument5 pagesDigital Image Processing and Soft Computing TechniquesSyed AshmadPas encore d'évaluation
- ERTOS Course OutcomesDocument2 pagesERTOS Course OutcomesSyed AshmadPas encore d'évaluation
- III - I R09 Regular Dec 2013Document162 pagesIII - I R09 Regular Dec 2013Syed AshmadPas encore d'évaluation
- III - I R09 Regular Dec 2013Document162 pagesIII - I R09 Regular Dec 2013Syed AshmadPas encore d'évaluation
- An Image Processing Algorithm To Estimate Bone2017Document4 pagesAn Image Processing Algorithm To Estimate Bone2017Syed AshmadPas encore d'évaluation
- DDVLECEDocument11 pagesDDVLECEakPas encore d'évaluation
- Automatic Identification of Fracture Region 2018 (2) - Annotated PDFDocument7 pagesAutomatic Identification of Fracture Region 2018 (2) - Annotated PDFSyed AshmadPas encore d'évaluation
- Digital Design Using Verilog HDL QBDocument2 pagesDigital Design Using Verilog HDL QBSyed AshmadPas encore d'évaluation
- Outcomes For I SemesterDocument2 pagesOutcomes For I SemesterSyed AshmadPas encore d'évaluation
- Digital Design Using Verilog HDL QBDocument14 pagesDigital Design Using Verilog HDL QBHarishReddyPas encore d'évaluation
- Memory Organization of the 8051 MicrocontrollerDocument4 pagesMemory Organization of the 8051 MicrocontrollerSyed AshmadPas encore d'évaluation
- Digital Image Processing and Soft Computing TechniquesDocument5 pagesDigital Image Processing and Soft Computing TechniquesSyed AshmadPas encore d'évaluation
- FPGA Logic Gates & Adder/Subtractor DesignDocument66 pagesFPGA Logic Gates & Adder/Subtractor DesignVishnu Brc57% (14)
- Digital Design Through Verilog HDLDocument1 pageDigital Design Through Verilog HDLSyed AshmadPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
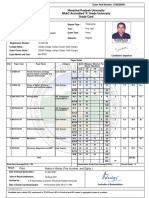
- Serial Number:1920110212668 Exam Roll Number Grade CardDocument2 pagesSerial Number:1920110212668 Exam Roll Number Grade Cardsimran vaidPas encore d'évaluation
- Parameter Adaptation of Reduced Order Models For Three-Dimensional Flutter AnalysisDocument9 pagesParameter Adaptation of Reduced Order Models For Three-Dimensional Flutter AnalysisAtsis PapadopoulosPas encore d'évaluation
- PROBABILITY ANALYSISDocument119 pagesPROBABILITY ANALYSISAnonymous bZtJlFvPtpPas encore d'évaluation
- Interference QuestionsDocument11 pagesInterference QuestionsKhaled SaadiPas encore d'évaluation
- Horizontal Twin-Shaft Paddle Mixers - The Ultimate in Mixing TechnologyDocument5 pagesHorizontal Twin-Shaft Paddle Mixers - The Ultimate in Mixing TechnologyMilling and Grain magazinePas encore d'évaluation
- 11 HW ChemistryDocument6 pages11 HW ChemistryJ BalanPas encore d'évaluation
- Design Modification of A Mechanical Footstep Power Generator Olive KaburuDocument56 pagesDesign Modification of A Mechanical Footstep Power Generator Olive KaburuDushyant HarnePas encore d'évaluation
- Misiulia-Angulo de Helice de EntradaDocument34 pagesMisiulia-Angulo de Helice de EntradaMiguel AnPas encore d'évaluation
- NSEP 2022-23 - (Questions and Answer)Document19 pagesNSEP 2022-23 - (Questions and Answer)Aditya KumarPas encore d'évaluation
- Surgical Lights and Operating Table SeriesDocument12 pagesSurgical Lights and Operating Table SeriesPABLO ZAMUDIOPas encore d'évaluation
- Product Note PD30 en RevA 2011 Anti-Sway Control ProgramDocument2 pagesProduct Note PD30 en RevA 2011 Anti-Sway Control ProgramkumarPas encore d'évaluation
- 1 BelzonaDocument41 pages1 BelzonashakeelahmadjsrPas encore d'évaluation
- Beam StandardDocument44 pagesBeam StandardweldmindPas encore d'évaluation
- Misfire Detection of A Turbocharged Diesel Engine by Using Artificial Neural NetworksDocument7 pagesMisfire Detection of A Turbocharged Diesel Engine by Using Artificial Neural NetworksJean Carlos PinedaPas encore d'évaluation
- Chapter 6 - Cementing - Part 1 PDFDocument32 pagesChapter 6 - Cementing - Part 1 PDFfadz607Pas encore d'évaluation
- Volumes by Cylindrical ShellsDocument7 pagesVolumes by Cylindrical Shellseomer1968Pas encore d'évaluation
- Catalog WefatermDocument55 pagesCatalog WefatermAlin NicolaePas encore d'évaluation
- Triton X 100Document2 pagesTriton X 100jelaapePas encore d'évaluation
- Ut Procedure 1Document8 pagesUt Procedure 1abhinavsmash66666Pas encore d'évaluation
- Phy WsDocument4 pagesPhy WsPranav VPas encore d'évaluation
- History of Representation TheoryDocument7 pagesHistory of Representation TheoryAaron HillmanPas encore d'évaluation
- (ISRM Book Series) Shunsuke Sakurai - Back Analysis in Rock Engineering-Routledge - CRC Press (2016) PDFDocument241 pages(ISRM Book Series) Shunsuke Sakurai - Back Analysis in Rock Engineering-Routledge - CRC Press (2016) PDFJorge Cortez CampañaPas encore d'évaluation
- Learning Objectives-2: Uniform MotionDocument7 pagesLearning Objectives-2: Uniform MotionBryanHarold BrooPas encore d'évaluation
- Abutment Design CalculationsDocument13 pagesAbutment Design CalculationsFitsum Abebe100% (1)
- 11P Trusses ProblemsDocument39 pages11P Trusses ProblemsHoward Johann Gomez VPas encore d'évaluation
- Instabilities and Nonequilibrium Structures VII & VIIIDocument377 pagesInstabilities and Nonequilibrium Structures VII & VIIIcoerenciacePas encore d'évaluation
- Check Samsung indoor unit LED errorsDocument84 pagesCheck Samsung indoor unit LED errorsbluerosedtuPas encore d'évaluation
- Venn Diagram Generator Academo - Org - Free, Interactive, EducationDocument1 pageVenn Diagram Generator Academo - Org - Free, Interactive, EducationChris DeBruyckerePas encore d'évaluation
- ZL - 205Document2 pagesZL - 205Fraz AhmadPas encore d'évaluation
- All Ceramic Material SelectionDocument6 pagesAll Ceramic Material SelectionERIKA BLANQUETPas encore d'évaluation