Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- AR06894-Vigileo UserManual 1LRDocument31 pagesAR06894-Vigileo UserManual 1LRsec.ivbPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
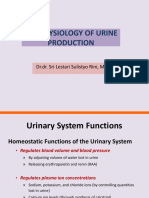
- The Physiology of Urine Production: DR - Dr. Sri Lestari Sulistyo Rini, MSCDocument89 pagesThe Physiology of Urine Production: DR - Dr. Sri Lestari Sulistyo Rini, MSCAkhmad FauzanPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Pranayama: The Serpent PowerDocument2 pagesPranayama: The Serpent PowermamoncinPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Muscular SystemDocument28 pagesMuscular SystemPridas GidPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- He Respiratory System in BabiesDocument16 pagesHe Respiratory System in BabiesWidiya Nur FatinahPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- L11 - Practice Q - HBDocument4 pagesL11 - Practice Q - HBEvan YEUNG [09N12]Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Body Fluids and Circulation NotesDocument8 pagesBody Fluids and Circulation Notessatyam6449Pas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Pathophysiology of HypothermiaDocument4 pagesPathophysiology of HypothermiaGracel QuiaotPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- SMK Green Road Term 2 Trial Exam 2019 MSDocument4 pagesSMK Green Road Term 2 Trial Exam 2019 MSvoon sjPas encore d'évaluation
- Pranayama Breathing Exercises GuideDocument16 pagesPranayama Breathing Exercises GuideHazel Aikulola GriffithPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- QP ICSE VII Bio RQB2Document3 pagesQP ICSE VII Bio RQB2sohail.shaikh5065Pas encore d'évaluation
- The Chemical Basis of Medical Climatolo (Y: Professor Giorgio PiccardiDocument6 pagesThe Chemical Basis of Medical Climatolo (Y: Professor Giorgio PiccardimarcelPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A&e Test - ATLSDocument14 pagesA&e Test - ATLSAnonymous x0P332K5uu86% (14)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Where To Place Your TENS PadsDocument8 pagesWhere To Place Your TENS PadsKailyne WatersPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Objectives: Pre-Analytical Considerations in PhlebotomyDocument9 pagesObjectives: Pre-Analytical Considerations in PhlebotomyMr. Potatohead100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Jem MusclesDocument11 pagesJem MusclesAnonymous CZAc9juPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Assessment: General Survey, Measurement, Vital SignsDocument10 pagesAssessment: General Survey, Measurement, Vital SignsNathan BarrerasPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- Class 1Document9 pagesClass 1The ExplorerPas encore d'évaluation
- Heart and blood vessels explained in detailDocument15 pagesHeart and blood vessels explained in detailIDKPas encore d'évaluation
- Autonomic Nervous System AnatomyDocument10 pagesAutonomic Nervous System AnatomyghalyPas encore d'évaluation
- KSMS Quarterly Exam BiologyDocument4 pagesKSMS Quarterly Exam BiologySumitaPas encore d'évaluation
- 7 Essential Steps of CPRDocument2 pages7 Essential Steps of CPRBea YmsnPas encore d'évaluation
- International Journal of Scientific Research: AnesthesiologyDocument2 pagesInternational Journal of Scientific Research: AnesthesiologyALfuPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Nervous System: Sensory PhysiologyDocument6 pagesThe Nervous System: Sensory Physiologyanon100% (1)
- Types and Causes of ShockDocument18 pagesTypes and Causes of ShockGaurav ChauhanPas encore d'évaluation
- HAP Question Paper Solution D. PharmaDocument9 pagesHAP Question Paper Solution D. PharmaSinger Rahul Sharma100% (1)
- Unconscious: By: Simranpreet KaurDocument12 pagesUnconscious: By: Simranpreet Kaurpreet kaurPas encore d'évaluation
- HypernatremiaDocument2 pagesHypernatremiaAliyah PundagPas encore d'évaluation
- Secrets To Effective and Holistic Asthma ControlDocument77 pagesSecrets To Effective and Holistic Asthma Controlrobert limPas encore d'évaluation
- Grade 11 .. Life Sciences TOPIC TEST: Gaseous Exchange: Learners NameDocument5 pagesGrade 11 .. Life Sciences TOPIC TEST: Gaseous Exchange: Learners Namedeveloping habit and lifestyle of praise and worshPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)