Vous aimerez peut-être aussi
- B.O. No. 1 S. 2023Document3 pagesB.O. No. 1 S. 2023edvince mickael bagunas sinonPas encore d'évaluation
- SAMPLE BNAP 2023 2025 - Template 1Document45 pagesSAMPLE BNAP 2023 2025 - Template 1Maryde Ompoy100% (3)
- Usapan PDFDocument51 pagesUsapan PDFPerry Bear100% (1)
- Brgy. Resolution For AdolescentDocument4 pagesBrgy. Resolution For AdolescentGina Salvador - GonzalesPas encore d'évaluation
- Executive Order No. 2019 - 21 (Dengue) For Other BarangayDocument4 pagesExecutive Order No. 2019 - 21 (Dengue) For Other BarangayGer Vin Meine VidadPas encore d'évaluation
- DILG Full Disclosure PolicyDocument6 pagesDILG Full Disclosure PolicyHelen FabraPas encore d'évaluation
- 05-S-2019 Dengue Ordinance of Barangay San CarlosDocument6 pages05-S-2019 Dengue Ordinance of Barangay San CarlosRonel Rosal MalunesPas encore d'évaluation
- E.O Anti Dengue CommitteeDocument3 pagesE.O Anti Dengue CommitteePao Lonzaga100% (1)
- Resolution For Adoptions at BrgyDocument4 pagesResolution For Adoptions at BrgyAedrian MacawiliPas encore d'évaluation
- Ordinance On BCPC IncentivesDocument8 pagesOrdinance On BCPC IncentivesNald CervasPas encore d'évaluation
- 09-2014 Adopting The Philippine Plan of Action For Nutrition.Document2 pages09-2014 Adopting The Philippine Plan of Action For Nutrition.SbGuinobatanPas encore d'évaluation
- Executive Order Anti DengueDocument2 pagesExecutive Order Anti Denguemichael bebayo100% (2)
- Barangay FDPDocument17 pagesBarangay FDPCarlo Torres100% (1)
- Barangay 8 Poblacion: Republic of The Philippines Tigbauan, IloiloDocument1 pageBarangay 8 Poblacion: Republic of The Philippines Tigbauan, IloiloFame LimPas encore d'évaluation
- REPUBLIC ACT No 11148Document15 pagesREPUBLIC ACT No 11148Ann Manalocon100% (1)
- EO No.-31 s.2013 Anti-Rabies CouncilDocument5 pagesEO No.-31 s.2013 Anti-Rabies Councilmaryson primo100% (1)
- BUBUATANHealth Board Plan July 2020Document4 pagesBUBUATANHealth Board Plan July 2020Mark Jake RodriguezPas encore d'évaluation
- BCPC E.O. No. 01 S. 2019Document2 pagesBCPC E.O. No. 01 S. 2019Barangay Taguitic100% (1)
- Eo An Executive Order Mandating The Establishment Maintenace Sustainability of Community GardenDocument1 pageEo An Executive Order Mandating The Establishment Maintenace Sustainability of Community GardenErickson PinedaPas encore d'évaluation
- 020 - 2022 - BNCDocument2 pages020 - 2022 - BNCIinday Anrym100% (1)
- Executive Order No. 02-2021 Implementing Team RPRH LawDocument2 pagesExecutive Order No. 02-2021 Implementing Team RPRH LawLyn Tabelisma OzarPas encore d'évaluation
- Eo LCPCDocument5 pagesEo LCPCXerxes F Batralo100% (2)
- Brgy Ordinancebcpc InstitutionalizationDocument5 pagesBrgy Ordinancebcpc InstitutionalizationAileen Labastida BarcenasPas encore d'évaluation
- "An Order Establishing The Implementing Team Fo The ResponsibleDocument5 pages"An Order Establishing The Implementing Team Fo The ResponsibleBarangay CatoPas encore d'évaluation
- BNC MtgMinutes 5-18-20Document4 pagesBNC MtgMinutes 5-18-20Jerrylyn MedinaPas encore d'évaluation
- d8 Minutes2014-03-25Document2 pagesd8 Minutes2014-03-25api-246926759Pas encore d'évaluation
- Compliance Report For Vaw DeskDocument6 pagesCompliance Report For Vaw Deskbarangay artacho1964 bautista100% (1)
- Ordinance On Vawc DeskDocument5 pagesOrdinance On Vawc DeskGuindapunan West Carigara LeytePas encore d'évaluation
- SB Resolution PPAN Adoption 2017-2022Document3 pagesSB Resolution PPAN Adoption 2017-2022Babuu BabuuPas encore d'évaluation
- PB Tasks & Responsibilities ChecklistDocument64 pagesPB Tasks & Responsibilities ChecklistLouie C. Manarpiis100% (3)
- Re-Organizing The Barangay Council For The Protection of ChildrenDocument4 pagesRe-Organizing The Barangay Council For The Protection of Childrenrogelio baltazarPas encore d'évaluation
- Barangay Nutrition Month Action Plan SilongonDocument11 pagesBarangay Nutrition Month Action Plan SilongonSimoneides MacahisPas encore d'évaluation
- Barangay Nutrition Committe: Project ProposalDocument3 pagesBarangay Nutrition Committe: Project ProposalDesiree OngPas encore d'évaluation
- Republic of The Philippines Province of Isabela Municipality of Gamu BARANGAY - Office of The Punong BarangayDocument2 pagesRepublic of The Philippines Province of Isabela Municipality of Gamu BARANGAY - Office of The Punong BarangayMarie AlejoPas encore d'évaluation
- Eo-Barangay Nutrition CommitteeDocument2 pagesEo-Barangay Nutrition CommitteeMaulawin Pagsanjan100% (1)
- Certification: Republic of The Philippines Province of Laguna City of Calamba Barangay La MesaDocument6 pagesCertification: Republic of The Philippines Province of Laguna City of Calamba Barangay La MesaBarangay La MesaPas encore d'évaluation
- Executive Order No. 032 S. 2022Document2 pagesExecutive Order No. 032 S. 2022SAMMY SARMIENTO100% (1)
- BNC Resolution Adopting Ra 10028Document2 pagesBNC Resolution Adopting Ra 10028Jocelyn Manao100% (1)
- 1000 DaysDocument1 page1000 DaysBob Joe100% (1)
- Ao 2014-09 BNCDocument2 pagesAo 2014-09 BNCapi-246926759100% (1)
- Ao 2014-03 BDCDocument2 pagesAo 2014-03 BDCapi-246926759100% (2)
- Pabasa Sa Nutrisyon' As One of The City's Key Programs On NutritionDocument2 pagesPabasa Sa Nutrisyon' As One of The City's Key Programs On NutritionTrixie Mae Umali100% (1)
- 017-2022-BHW SignedDocument3 pages017-2022-BHW SignedIinday Anrym100% (1)
- Resolution 2022Document15 pagesResolution 2022Charlene Miguel100% (1)
- EO-HAPAG BRGY. Pob. SurDocument2 pagesEO-HAPAG BRGY. Pob. SurRitchie BalberonaPas encore d'évaluation
- ZODDocument15 pagesZODJudyLynPas encore d'évaluation
- 24 BgfpsDocument2 pages24 Bgfpsyan deePas encore d'évaluation
- 04-1-2014 MinutesDocument2 pages04-1-2014 MinutesJasielMendozaPas encore d'évaluation
- Activity Design - ADAC StrengtheningDocument3 pagesActivity Design - ADAC StrengtheningRee MaslogPas encore d'évaluation
- LSCRDocument15 pagesLSCRmaui hPas encore d'évaluation
- LSCR ReportDocument10 pagesLSCR ReportCpu Silang100% (1)
- GAD Plan & Accomplishment 2021Document5 pagesGAD Plan & Accomplishment 2021Yuri Villanueva100% (1)
- Barangay RPRH-LawDocument3 pagesBarangay RPRH-Lawelyss100% (4)
- Dtp. Barangay Sta MariaDocument29 pagesDtp. Barangay Sta MariaDonavel Nodora JojuicoPas encore d'évaluation
- 6 - BeswmcDocument3 pages6 - Beswmcsan nicolas 2nd betis guagua pampangaPas encore d'évaluation
- Republic of The Philippines Province of Bulacan Municipality of Pulilan Barangay Poblacion Office of The Punong BarangayDocument2 pagesRepublic of The Philippines Province of Bulacan Municipality of Pulilan Barangay Poblacion Office of The Punong BarangayJustine CandelariaPas encore d'évaluation
- Trainers’ Manual on Facilitating Local Government-Led Community-Driven DevelopmentD'EverandTrainers’ Manual on Facilitating Local Government-Led Community-Driven DevelopmentPas encore d'évaluation
- PA00WKKNDocument490 pagesPA00WKKNRima SumayyahPas encore d'évaluation
- Who SopDocument48 pagesWho SopAadityaa PawarPas encore d'évaluation
- Family Planning in The Hospital Operational Guide For Recording and Reporting PDFDocument69 pagesFamily Planning in The Hospital Operational Guide For Recording and Reporting PDFViolet CherryPas encore d'évaluation
- Sequalae of Wearing Complete DenturesDocument34 pagesSequalae of Wearing Complete DenturesAyeshaAslamPas encore d'évaluation
- Intradermal Delivery Vaccines Report 2009 SeptDocument94 pagesIntradermal Delivery Vaccines Report 2009 SeptSantoso CokroPas encore d'évaluation
- Allysa Marie Silbol Beed I1Document3 pagesAllysa Marie Silbol Beed I1Allysa Marie SilbolPas encore d'évaluation
- KET4Document7 pagesKET4Janetta RheaPas encore d'évaluation
- Daftar PustakaDocument37 pagesDaftar PustakaprilaPas encore d'évaluation
- Top Muscle Building and Weight Gain SecretsDocument8 pagesTop Muscle Building and Weight Gain SecretsKarl Gallagher83% (6)
- An Overview of The Role of Nurses and Midwives in Leadership and Management in EuropeDocument44 pagesAn Overview of The Role of Nurses and Midwives in Leadership and Management in EuropeTCPas encore d'évaluation
- Cultural Competence or Cultural Humility Moving Beyond The DebateDocument4 pagesCultural Competence or Cultural Humility Moving Beyond The DebateEstela MedinaPas encore d'évaluation
- Small Changes, Big Results, Revised and UpdatedDocument18 pagesSmall Changes, Big Results, Revised and UpdatedThe Recipe Club100% (1)
- Management Hypovolemic Shock, NurinDocument12 pagesManagement Hypovolemic Shock, Nurinرفاعي آكرمPas encore d'évaluation
- A Client With Cushing's Syndrome: Nursing Care PlanDocument1 pageA Client With Cushing's Syndrome: Nursing Care PlanJulius Caesar ColladoPas encore d'évaluation
- Ensaio Clínico - Rivaroxaban Vs Warfarin in High-Risk Patients WithDocument7 pagesEnsaio Clínico - Rivaroxaban Vs Warfarin in High-Risk Patients WithesdrasPas encore d'évaluation
- RRL On HospitalsDocument13 pagesRRL On HospitalsNellyn GutierrezPas encore d'évaluation
- 002 - 1203 - Ni Wayan Ari Anindita Sari - GalleyDocument5 pages002 - 1203 - Ni Wayan Ari Anindita Sari - GalleyHaningtyas IndahPas encore d'évaluation
- Food AdjunctDocument15 pagesFood AdjunctRoby martinus bayaPas encore d'évaluation
- FISPQ - Sodium-CarbonateDocument12 pagesFISPQ - Sodium-CarbonateJaqueline GarciaPas encore d'évaluation
- Nursing Home Abuse - A Rising Threat in The USDocument8 pagesNursing Home Abuse - A Rising Threat in The USLezDo techmed LLCPas encore d'évaluation
- 4832 Concept Map On Failure To Thrive-Desktop-1dptoe6Document11 pages4832 Concept Map On Failure To Thrive-Desktop-1dptoe6api-603346045Pas encore d'évaluation
- Chronic Renal Failure Nursing Care PlanDocument6 pagesChronic Renal Failure Nursing Care PlanRuva Oscass JimmyPas encore d'évaluation
- Jaundice: From Superstition To ScienceDocument93 pagesJaundice: From Superstition To ScienceDr Muhammad ShoyabPas encore d'évaluation
- Cmca Activity 1 AliamenDocument5 pagesCmca Activity 1 AliamenJasmine AliamenPas encore d'évaluation
- Heutagogy Learning Beyond The Classroom Vijaya Bhanu IndiaDocument24 pagesHeutagogy Learning Beyond The Classroom Vijaya Bhanu IndiaVijayaBhanuKotePas encore d'évaluation
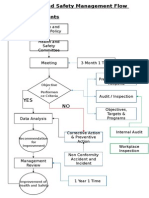
- Health and Safety FlowDocument6 pagesHealth and Safety Flowzaki0304Pas encore d'évaluation
- Annotated BibliographyDocument12 pagesAnnotated Bibliographyapi-408297855Pas encore d'évaluation
- Vasculitis When To Consider This DiagnosisDocument15 pagesVasculitis When To Consider This DiagnosisAndres PortesPas encore d'évaluation
- DNBDocument20 pagesDNBRaghavendra NalatawadPas encore d'évaluation
- NIH Document Production Cover Letter 2021.10.20 McMorris RodgersDocument2 pagesNIH Document Production Cover Letter 2021.10.20 McMorris RodgersAl StatiliusPas encore d'évaluation
- Research Essay Final DraftDocument14 pagesResearch Essay Final Draftapi-558668635Pas encore d'évaluation
- CDEM 17jan Complete WEBDocument24 pagesCDEM 17jan Complete WEBRicardo Jonathan Ayala GarciaPas encore d'évaluation
- 2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsDocument10 pages2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsSittie Haneen TabaraPas encore d'évaluation