Vous aimerez peut-être aussi
- Bajaj Allianz Cashless Request FormDocument3 pagesBajaj Allianz Cashless Request FormM/s MicrotechPas encore d'évaluation
- The Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Document4 pagesThe Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Mcnet WidePas encore d'évaluation
- National Inurance Company Limited - Claim FormDocument3 pagesNational Inurance Company Limited - Claim FormfuckyouprettyPas encore d'évaluation
- Claim FormDocument3 pagesClaim FormKhameer L Shah100% (1)
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationHarold TanPas encore d'évaluation
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationFirmament DevelopmentPas encore d'évaluation
- In-Patient Claim FormDocument2 pagesIn-Patient Claim Formfaisal_1241Pas encore d'évaluation
- Cashless Request FormDocument4 pagesCashless Request FormManish RanjanPas encore d'évaluation
- Claim Form IHealthcareDocument5 pagesClaim Form IHealthcarePradeep Kumar VupalaPas encore d'évaluation
- Claims Reimbursement Form (For MRC) : Member General InformationDocument2 pagesClaims Reimbursement Form (For MRC) : Member General Informationathenixia100% (1)
- Adamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormDocument2 pagesAdamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormubaidPas encore d'évaluation
- Details of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument5 pagesDetails of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ASumitThoratPas encore d'évaluation
- NAIC Claim Form PDFDocument3 pagesNAIC Claim Form PDFMohit BaggaPas encore d'évaluation
- Health Insurance Claim FormDocument3 pagesHealth Insurance Claim FormdivechahimanshuPas encore d'évaluation
- OIC Claim FormDocument4 pagesOIC Claim FormPrashant SinghPas encore d'évaluation
- The New India Assurance Company Limited: Claim NumberDocument3 pagesThe New India Assurance Company Limited: Claim Numberharshmanu1612Pas encore d'évaluation
- ClaimDocument1 pageClaimStephen JoyPas encore d'évaluation
- GMC Claim Form How To File A ClaimDocument4 pagesGMC Claim Form How To File A ClaimtweetknotPas encore d'évaluation
- Claims Form For New India AssuranceDocument2 pagesClaims Form For New India AssuranceRafael BlackPas encore d'évaluation
- Others Claim FormDocument5 pagesOthers Claim FormArvind RayPas encore d'évaluation
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDeepakPas encore d'évaluation
- Tata AIA Life Insurance Company Limited: Total & Permanent Disability Claim FormDocument2 pagesTata AIA Life Insurance Company Limited: Total & Permanent Disability Claim FormPrashob SugathanPas encore d'évaluation
- Bajaj Claim FormDocument9 pagesBajaj Claim FormYogi’s iphone Pas encore d'évaluation
- Medical Claim Form (Reimbursement Only)Document2 pagesMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- Claim FormDocument3 pagesClaim FormSumit ManglaniPas encore d'évaluation
- Icici Lombard Health Care Insurance Claim FormDocument5 pagesIcici Lombard Health Care Insurance Claim FormsperoPas encore d'évaluation
- CFPA-Medical ExpensesDocument2 pagesCFPA-Medical ExpensesDivya VoletiPas encore d'évaluation
- 30 Medicl Procdur For ClaimDocument7 pages30 Medicl Procdur For Claimبلال خالدPas encore d'évaluation
- Kolkata Claim Form - MD-IndiaDocument4 pagesKolkata Claim Form - MD-Indiadipankar0majumderPas encore d'évaluation
- Medical Reibursement Proposal Form SetDocument5 pagesMedical Reibursement Proposal Form SetSharath VaddiparthiPas encore d'évaluation
- Claims Reimbursement Form PDFDocument2 pagesClaims Reimbursement Form PDFokong bokongPas encore d'évaluation
- ChecklistDocument9 pagesChecklistkarthikfuser0183Pas encore d'évaluation
- 14) ELIB-Female CI-Claim FormDocument7 pages14) ELIB-Female CI-Claim Formbibianna93Pas encore d'évaluation
- Reimbursement Form - GamayonDocument2 pagesReimbursement Form - Gamayonreese93Pas encore d'évaluation
- Accident Claim Form UpdatedDocument5 pagesAccident Claim Form UpdatedWeen Keen LeePas encore d'évaluation
- Claim Form IHealthcareDocument6 pagesClaim Form IHealthcareHarish AdityaPas encore d'évaluation
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormShubakar ReddyPas encore d'évaluation
- Credential IngDocument13 pagesCredential Ingdr_rajatjainPas encore d'évaluation
- NSTUMP - Proposal FormDocument7 pagesNSTUMP - Proposal FormJagadeesh MaheshPas encore d'évaluation
- Medical Attendants Certificate17062019Document2 pagesMedical Attendants Certificate17062019PrathameshPas encore d'évaluation
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Document2 pagesMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviPas encore d'évaluation
- ICICI - Claim FormDocument5 pagesICICI - Claim FormRaja RamanPas encore d'évaluation
- Pre-Authorization Request Form: (Please Tick The Relevant Box)Document1 pagePre-Authorization Request Form: (Please Tick The Relevant Box)Pallavi ShuklaPas encore d'évaluation
- Medical FormDocument4 pagesMedical Formnki5Pas encore d'évaluation
- Forms PensionersDocument15 pagesForms PensionersAnimesh DasPas encore d'évaluation
- Nhif Universal Claim FormDocument2 pagesNhif Universal Claim Formmaoaweys hospital75% (4)
- PhilHealth ClaimForm2Document2 pagesPhilHealth ClaimForm2La Lolls CruzPas encore d'évaluation
- PhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Document2 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Chrysanthus HerreraPas encore d'évaluation
- ALAIN CAMPBELL, M.D. MASSACHUSETTS LICENSE APPLICATIONS Total As of 2015Document85 pagesALAIN CAMPBELL, M.D. MASSACHUSETTS LICENSE APPLICATIONS Total As of 2015Anonymous 8m05a5Pas encore d'évaluation
- Medicaid AppealDocument15 pagesMedicaid Appealmtp7389Pas encore d'évaluation
- Medical Reimbursement Form 2Document2 pagesMedical Reimbursement Form 2Rakesh KumarPas encore d'évaluation
- NPMP Parivar Proposal FormDocument8 pagesNPMP Parivar Proposal Formpradip nathujiPas encore d'évaluation
- Aon - Aia Ghs Claim Form - Oct 2014Document3 pagesAon - Aia Ghs Claim Form - Oct 2014John SmithPas encore d'évaluation
- Cross-Training: The Medical Assistant WorkbookD'EverandCross-Training: The Medical Assistant WorkbookPas encore d'évaluation
- Newman's Billing and Coding Technicians Study GuideD'EverandNewman's Billing and Coding Technicians Study GuideÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Newman's Medical Billing and Coding Technicians Study GuideD'EverandNewman's Medical Billing and Coding Technicians Study GuidePas encore d'évaluation
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsD'EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsPas encore d'évaluation
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!D'EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Évaluation : 1 sur 5 étoiles1/5 (1)
- Medical Coding: a QuickStudy Laminated Reference GuideD'EverandMedical Coding: a QuickStudy Laminated Reference GuidePas encore d'évaluation
- Speaker Session Review (Ali Qavi)Document1 pageSpeaker Session Review (Ali Qavi)AliPas encore d'évaluation
- Case Study 2 The Petronas Towers, Kuala LumpurDocument34 pagesCase Study 2 The Petronas Towers, Kuala LumpurAliPas encore d'évaluation
- MEGA PROJECT - Jumeirah Palm Island PDFDocument14 pagesMEGA PROJECT - Jumeirah Palm Island PDFAliPas encore d'évaluation
- 2006 Maglev ReducedDocument185 pages2006 Maglev ReducedAliPas encore d'évaluation
- Management Glossary - Musa KamawiDocument50 pagesManagement Glossary - Musa KamawiKazi Nazrul IslamPas encore d'évaluation
- Presentation - ASDA T&DDocument6 pagesPresentation - ASDA T&DAliPas encore d'évaluation
- Pakistan CPI Dec 2019Document3 pagesPakistan CPI Dec 2019AliPas encore d'évaluation
- List of Academic Institutions in PakistaDocument2 pagesList of Academic Institutions in Pakistamuqadam buttPas encore d'évaluation
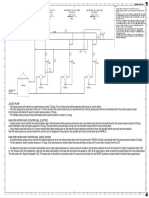
- Fire Water SystemDocument1 pageFire Water SystemAliPas encore d'évaluation
- CasesDocument1 pageCasesAliPas encore d'évaluation
- Management Glossary - Musa KamawiDocument50 pagesManagement Glossary - Musa KamawiKazi Nazrul IslamPas encore d'évaluation
- FRP Hdpe ComparisonDocument3 pagesFRP Hdpe ComparisonbcsmurthyPas encore d'évaluation
- Hub Bypass NHADocument58 pagesHub Bypass NHAAliPas encore d'évaluation
- Water Samples ReportDocument10 pagesWater Samples ReportAliPas encore d'évaluation
- 1001.C00 GEN Design Concept Rev00Document5 pages1001.C00 GEN Design Concept Rev00AliPas encore d'évaluation
- Grid Plan-Layout1Document1 pageGrid Plan-Layout1AliPas encore d'évaluation
- Mooring Forces Port or STBD On Quay WWW - Thenavalarch.com Rev 1Document10 pagesMooring Forces Port or STBD On Quay WWW - Thenavalarch.com Rev 1Mohamed Elfawal100% (1)
- TRF-342 CPHGCL Fca 28-07-2017 13078-80Document19 pagesTRF-342 CPHGCL Fca 28-07-2017 13078-80AliPas encore d'évaluation
- NIO Karwat Report 27 2 18Document26 pagesNIO Karwat Report 27 2 18AliPas encore d'évaluation
- Krwat Topo-Layout1Document1 pageKrwat Topo-Layout1AliPas encore d'évaluation
- State of Industry Report 2015Document228 pagesState of Industry Report 2015Muhammad Saulat AliPas encore d'évaluation
- Linked Ship Shore Emergency Shutdown Systems For Oil and Chemical TransfersDocument21 pagesLinked Ship Shore Emergency Shutdown Systems For Oil and Chemical Transfersjbloggs2007Pas encore d'évaluation
- 1001.C12 GEN93 SLD Rev00 2018-06-12 DRAFTDocument6 pages1001.C12 GEN93 SLD Rev00 2018-06-12 DRAFTAliPas encore d'évaluation
- Application of China Power Hub Generation Company Limited For Adjustment of Tariff For Optimal Jetty Design For Its 2x660 MW Imported Coal ProjectDocument30 pagesApplication of China Power Hub Generation Company Limited For Adjustment of Tariff For Optimal Jetty Design For Its 2x660 MW Imported Coal ProjectAliPas encore d'évaluation
- Valo Business Plan 7Document72 pagesValo Business Plan 7AliPas encore d'évaluation
- Kansai Paint Company ProfileDocument6 pagesKansai Paint Company ProfileAliPas encore d'évaluation
- Class Test EmotionsDocument1 pageClass Test EmotionsMEGHA SHARMAPas encore d'évaluation
- Procedural Checklist NCM 112 RLE Preparing A Sterile Field Opening A Sterile Pack Adding Items To A Sterile Field Adding Liquids To A Sterile Field Skin PreparationDocument5 pagesProcedural Checklist NCM 112 RLE Preparing A Sterile Field Opening A Sterile Pack Adding Items To A Sterile Field Adding Liquids To A Sterile Field Skin PreparationAbegail Eliah EstalanePas encore d'évaluation
- KP Neeraja: The Principles and Practice of Nurse EducationDocument6 pagesKP Neeraja: The Principles and Practice of Nurse EducationabcPas encore d'évaluation
- FullmanuscriptDocument3 pagesFullmanuscriptAmalia Tri UtamiPas encore d'évaluation
- Salus Pco HistoryDocument27 pagesSalus Pco HistoryVladislav StevanovicPas encore d'évaluation
- Substance Abuse BrochureDocument2 pagesSubstance Abuse Brochureapi-272566401Pas encore d'évaluation
- WebinabsDocument336 pagesWebinabssacin99999Pas encore d'évaluation
- Sickle CellDocument21 pagesSickle CellLeon0% (1)
- Osteomalasia GujaratiDocument4 pagesOsteomalasia Gujaratidhavalb20Pas encore d'évaluation
- Glycemic Index Vs LoadDocument3 pagesGlycemic Index Vs LoaddominantnaturePas encore d'évaluation
- Drug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument1 pageDrug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesJonna Mae TurquezaPas encore d'évaluation
- Pernicious Anemia - MitchDocument18 pagesPernicious Anemia - Mitchthalafuj100% (1)
- Community Medicine Tranx (Family Medicine)Document13 pagesCommunity Medicine Tranx (Family Medicine)Kaye NeePas encore d'évaluation
- Topical Lotion Formulation PDFDocument45 pagesTopical Lotion Formulation PDFMustafa ArarPas encore d'évaluation
- Menastil Complete Clinical Trials - Pain Relief That Works.Document43 pagesMenastil Complete Clinical Trials - Pain Relief That Works.emoryholstPas encore d'évaluation
- Classification of Mental Disorder, Antisocial Personalities, Drug and Alcohol DependenceDocument15 pagesClassification of Mental Disorder, Antisocial Personalities, Drug and Alcohol DependenceAdrian SingsonPas encore d'évaluation
- Soal Bahasa Inggris - Evaluasi TestDocument9 pagesSoal Bahasa Inggris - Evaluasi TestHamdani IlhamPas encore d'évaluation
- Rs Pena 98 Jl. Pemuda Pengasinan N0.36 Kec Gn. Sindur Bogor Telp: (021) 7587 4401,-FaxDocument61 pagesRs Pena 98 Jl. Pemuda Pengasinan N0.36 Kec Gn. Sindur Bogor Telp: (021) 7587 4401,-Faxrichard fernandoPas encore d'évaluation
- Adilah TranskripDocument1 pageAdilah Transkripadik_mira893219Pas encore d'évaluation
- Drug-Induced Nutrient DepletionDocument4 pagesDrug-Induced Nutrient DepletionVictoria HristovaPas encore d'évaluation
- VancomycinDocument2 pagesVancomycinRye AnchPas encore d'évaluation
- Euthanasia Methods For Dogs and CatsDocument3 pagesEuthanasia Methods For Dogs and Catssharath_mbPas encore d'évaluation
- CV - Updated April 2023Document6 pagesCV - Updated April 2023api-641524095Pas encore d'évaluation
- The Anatomical Record - 2021 - Vater - The Topographic and Systematic Anatomy of The Alpaca StomachDocument15 pagesThe Anatomical Record - 2021 - Vater - The Topographic and Systematic Anatomy of The Alpaca StomachMai Chi PhạmPas encore d'évaluation
- StetDocument34 pagesStetCameron FoxPas encore d'évaluation
- DR Kshitij ResumeDocument3 pagesDR Kshitij ResumeBarney StinsonPas encore d'évaluation
- Beneficence and Non-MaleficenceDocument3 pagesBeneficence and Non-MaleficenceRathin BanerjeePas encore d'évaluation
- Cramp Pages 1Document10 pagesCramp Pages 1masi10Pas encore d'évaluation
- Using A Handheld Resuscitation Bag and MaskDocument2 pagesUsing A Handheld Resuscitation Bag and MaskLhara Vhaneza CuetoPas encore d'évaluation
- Proliferative EndometriumDocument4 pagesProliferative EndometriumKristine Dela CruzPas encore d'évaluation