Vous aimerez peut-être aussi
- Article: Brain Injury Unmasking Ehlers-Danlos Syndromes After TrauDocument17 pagesArticle: Brain Injury Unmasking Ehlers-Danlos Syndromes After TrauGèniaPas encore d'évaluation
- Eds Murcia 2015Document36 pagesEds Murcia 2015GèniaPas encore d'évaluation
- Article: Brain Injury Unmasking Ehlers-Danlos Syndromes After TrauDocument17 pagesArticle: Brain Injury Unmasking Ehlers-Danlos Syndromes After TrauGèniaPas encore d'évaluation
- CND - Further Organic Abnormalities in CFIDSDocument9 pagesCND - Further Organic Abnormalities in CFIDSGèniaPas encore d'évaluation
- Orthostatic Intolerance and Chronic Fat... Hlers-Danlos Syndrome. - PubMed - NCBIDocument2 pagesOrthostatic Intolerance and Chronic Fat... Hlers-Danlos Syndrome. - PubMed - NCBIGèniaPas encore d'évaluation
- From Ignorance To Denial About An Orphan, But No Rare, Genetic Disease: Ehlers-Danlos Syndrome (EDS Type III)Document6 pagesFrom Ignorance To Denial About An Orphan, But No Rare, Genetic Disease: Ehlers-Danlos Syndrome (EDS Type III)GèniaPas encore d'évaluation
- Chronic Fatigue in Ehlers-Danlos Syndrome-Hypermobile Type-Hakim Et Al-2017-American Journal of Medical Genetics Part C - Seminars in Medical GeneticsDocument6 pagesChronic Fatigue in Ehlers-Danlos Syndrome-Hypermobile Type-Hakim Et Al-2017-American Journal of Medical Genetics Part C - Seminars in Medical GeneticsGèniaPas encore d'évaluation
- Jaekle EDS and PregnancyDocument35 pagesJaekle EDS and PregnancyGèniaPas encore d'évaluation
- Professor Claude Hamonet's Website - SE... and Access To Diagnosis QuestionnaireDocument8 pagesProfessor Claude Hamonet's Website - SE... and Access To Diagnosis QuestionnaireGèniaPas encore d'évaluation
- Eds Diagnostic ToolDocument27 pagesEds Diagnostic ToolGènia100% (1)
- A Novel Mutation Screening System For E... Tion With Small Amp... - PubMed - NCBIDocument2 pagesA Novel Mutation Screening System For E... Tion With Small Amp... - PubMed - NCBIGèniaPas encore d'évaluation
- Eds Syndrome or DiseaseDocument5 pagesEds Syndrome or DiseaseGèniaPas encore d'évaluation
- CND - Further Organic Abnormalities in CFIDSDocument9 pagesCND - Further Organic Abnormalities in CFIDSGèniaPas encore d'évaluation
- Too Tired EDS and Fatigue - Brad TinkleDocument34 pagesToo Tired EDS and Fatigue - Brad TinkleGèniaPas encore d'évaluation
- Joint Mobility and EdsDocument5 pagesJoint Mobility and EdsGèniaPas encore d'évaluation
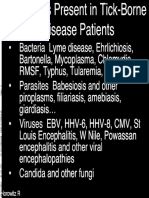
- Vectors of LymeDocument3 pagesVectors of LymeGèniaPas encore d'évaluation
- McsconsensusDocument6 pagesMcsconsensusGèniaPas encore d'évaluation
- Forced To Disconnect - ES Refugees in Sweden Ladberge 2008Document70 pagesForced To Disconnect - ES Refugees in Sweden Ladberge 2008EMFsafetyPas encore d'évaluation
- DR Pocinki EDSAwareness2016 PDFDocument58 pagesDR Pocinki EDSAwareness2016 PDFGènia100% (2)
- Alan PocinkiDocument33 pagesAlan PocinkiGèniaPas encore d'évaluation
- The Clinical and Scientific Basis of Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome Byron M. Hyde, M.D.Document753 pagesThe Clinical and Scientific Basis of Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome Byron M. Hyde, M.D.Gènia100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- NarrativeDocument2 pagesNarrativeRomel LeoPas encore d'évaluation
- Continuous chromatographic separation technologies for glucose syrup processesDocument6 pagesContinuous chromatographic separation technologies for glucose syrup processesAriel LopezPas encore d'évaluation
- Investigation On Cold Drinks For The Presence of Alcohol ...Document20 pagesInvestigation On Cold Drinks For The Presence of Alcohol ...Umair Husain100% (1)
- Internship ReportDocument62 pagesInternship Reportmaqsoodahmad_ftPas encore d'évaluation
- 12 Common Myths Facts On Honey EbookDocument30 pages12 Common Myths Facts On Honey EbookMira SabriPas encore d'évaluation
- NDT ReviewerDocument111 pagesNDT ReviewerMay RodeoPas encore d'évaluation
- Hala HaramDocument17 pagesHala Haramsweetie-PeanutsPas encore d'évaluation
- 10thedition Spring 2022Document107 pages10thedition Spring 2022UMAR FARIDIPas encore d'évaluation
- Alana Pascal - Kombucha - How-To and What It's All AboutDocument125 pagesAlana Pascal - Kombucha - How-To and What It's All Aboutjeesup9100% (4)
- CHE 31 Chemical Engineering CalculationsDocument13 pagesCHE 31 Chemical Engineering CalculationsxxkooonxxPas encore d'évaluation
- Sweet Truth: Not All Carbohydrates Are Alike: National Center For Case Study Teaching in ScienceDocument6 pagesSweet Truth: Not All Carbohydrates Are Alike: National Center For Case Study Teaching in ScienceDiana Limoran NeriPas encore d'évaluation
- Raw Food EbookDocument33 pagesRaw Food Ebookzimaios100% (2)
- Module in Carbohydrates PDFDocument19 pagesModule in Carbohydrates PDFAndreiPas encore d'évaluation
- Unit 1 CarbohydratesDocument99 pagesUnit 1 CarbohydratesRameshbabuPas encore d'évaluation
- Artisan Distilling - A Guide For Small DistilleriesDocument102 pagesArtisan Distilling - A Guide For Small DistilleriespixtaccioPas encore d'évaluation
- Separation of Carbohydrates in Dairy Products by High Performance Liquid Chromatography 1Document7 pagesSeparation of Carbohydrates in Dairy Products by High Performance Liquid Chromatography 1KhalidPas encore d'évaluation
- Biochemistry Pacop PinkgreenDocument28 pagesBiochemistry Pacop PinkgreenQueenPas encore d'évaluation
- Science 10 CarbohydratesDocument4 pagesScience 10 Carbohydrateskarizajean desalisaPas encore d'évaluation
- Expert Fat Loss GuideDocument66 pagesExpert Fat Loss GuideAmanda Rutllant100% (2)
- Weight Loss Cures PrintDocument272 pagesWeight Loss Cures PrintLee0% (2)
- Oten BiologyDocument798 pagesOten BiologyZarinaPas encore d'évaluation
- Effect of Sugar Substitute On Sucrose Crystal Growth Rate PDFDocument6 pagesEffect of Sugar Substitute On Sucrose Crystal Growth Rate PDFFelipe RiveraPas encore d'évaluation
- Food Labels: "By Law, Food Labels Must Be True. But Manufacturers Can Pick and Choose Which Facts To Highlight and Spin."Document8 pagesFood Labels: "By Law, Food Labels Must Be True. But Manufacturers Can Pick and Choose Which Facts To Highlight and Spin."KrzysztofRosaPas encore d'évaluation
- Chemistry Project:: Analysis of HoneyDocument16 pagesChemistry Project:: Analysis of HoneyDARKRAI GAMINGPas encore d'évaluation
- Effect of PH On Non-Enzymatic Browning Reaction DuringDocument8 pagesEffect of PH On Non-Enzymatic Browning Reaction DuringYazwar KotoPas encore d'évaluation
- PBL ReportDocument15 pagesPBL Reportjem70Pas encore d'évaluation
- What is Jaggery? The Sweet Traditional Sugar ExplainedDocument20 pagesWhat is Jaggery? The Sweet Traditional Sugar ExplainedWaleed IjazPas encore d'évaluation
- Protoplasm - Basis of All LifeDocument10 pagesProtoplasm - Basis of All LifeRaisa Jewell BustoPas encore d'évaluation
- 4 & 5 (Chemical Composition, Metabolism & Enzymes)Document12 pages4 & 5 (Chemical Composition, Metabolism & Enzymes)Jia YuePas encore d'évaluation
- Nutrition Exam I Sample QuestionsAnswers! - by Ramesh C. ReddyDocument6 pagesNutrition Exam I Sample QuestionsAnswers! - by Ramesh C. ReddyRukaya tibilPas encore d'évaluation