Vous aimerez peut-être aussi
- Heart Failure Care PlanDocument6 pagesHeart Failure Care PlanOlivia Winkler StuartPas encore d'évaluation
- 5 Nursing Diagnoses and Interventions for HypertensionDocument7 pages5 Nursing Diagnoses and Interventions for Hypertensionmelerine16Pas encore d'évaluation
- Osteomalacia Care Plan/OthersDocument11 pagesOsteomalacia Care Plan/OthersJill Jackson, RNPas encore d'évaluation
- Thoracocentasis: INTRODUCTION:-Thoracentasis Also Known As The Thoracocentasis or Plural Tap Is AnDocument7 pagesThoracocentasis: INTRODUCTION:-Thoracentasis Also Known As The Thoracocentasis or Plural Tap Is AnaparnaPas encore d'évaluation
- Cardiovascular Assessment: Assessment Uses of CVS AssessmentDocument8 pagesCardiovascular Assessment: Assessment Uses of CVS AssessmentKawaljit KaurPas encore d'évaluation
- Care Plan Unstable AnginaDocument4 pagesCare Plan Unstable Anginaالغزال الذهبي50% (6)
- Nursing Care PlanDocument15 pagesNursing Care PlanZhel Geron MercadoPas encore d'évaluation
- Nursing Care Plan for TonsillitisDocument3 pagesNursing Care Plan for TonsillitisEden Cruz50% (6)
- NCP PTBDocument2 pagesNCP PTBKath TalubanPas encore d'évaluation
- Section P - Group 1 E.C.S. - Pediatric Ward Mr. Ralph P. Pilapil, R.N. Clinical InstructorDocument62 pagesSection P - Group 1 E.C.S. - Pediatric Ward Mr. Ralph P. Pilapil, R.N. Clinical InstructorClaudine N SantillanPas encore d'évaluation
- Care of Patients With Mechanical VentilatorDocument4 pagesCare of Patients With Mechanical VentilatorIman Bee Sanayon0% (1)
- Nursing Care Plan Problem: Difficulty of BreathingDocument5 pagesNursing Care Plan Problem: Difficulty of BreathingIvan Louise Fajardo ManiquizPas encore d'évaluation
- Postural DrainageDocument6 pagesPostural DrainageKit Alizon Barredo0% (1)
- Managing Arteriosclerosis with Nursing CareDocument6 pagesManaging Arteriosclerosis with Nursing CareANCHAL SHARMAPas encore d'évaluation
- Nursing Care Plan - 1 AlyanaDocument1 pageNursing Care Plan - 1 AlyanaKen100% (1)
- Bronchial Hygiene Therapy ElectiveDocument20 pagesBronchial Hygiene Therapy ElectiveHelen Grace Dela Cruz0% (1)
- CP Intestinal Obstruction Nursing Care PlanDocument7 pagesCP Intestinal Obstruction Nursing Care PlanShiella Heart MalanaPas encore d'évaluation
- Preoperative Teaching EssentialsDocument11 pagesPreoperative Teaching EssentialsDani ThomasPas encore d'évaluation
- Nursing Care PlanDocument4 pagesNursing Care PlanJoshua Pascasio100% (1)
- Nursing Care Plan Renal FailureDocument2 pagesNursing Care Plan Renal FailureMark Jason Rabadan100% (1)
- Nursing Diagnosis For Coronary Artery Disease - Acute PainDocument2 pagesNursing Diagnosis For Coronary Artery Disease - Acute PainAngie Mandeoya100% (1)
- Nursing Care PlansDocument22 pagesNursing Care PlansAnonymous 0C4OZmR0% (1)
- Nursing Care Plan Congestive Heart FailureDocument2 pagesNursing Care Plan Congestive Heart FailureRalph Dumawaa60% (5)
- Cardiac System AssessmentDocument14 pagesCardiac System AssessmentValarmathi100% (1)
- NGT LavageDocument16 pagesNGT LavageTina Alteran100% (1)
- NCP PancreatitisDocument2 pagesNCP PancreatitisJeanelle GenerosoPas encore d'évaluation
- Oxygen InhalationDocument32 pagesOxygen Inhalationvarshasharma05100% (3)
- Hyperthyroidism N C P BY BHERU LALDocument1 pageHyperthyroidism N C P BY BHERU LALBheru Lal100% (1)
- NCP Heart BlockDocument3 pagesNCP Heart BlockEköw Santiago Javier33% (3)
- Status Asthmaticus: Severe Persistent AsthmaDocument2 pagesStatus Asthmaticus: Severe Persistent Asthmahemaanandhy0% (1)
- Liver Cirrhosis Nursing Care PlansDocument17 pagesLiver Cirrhosis Nursing Care Plansmarsan12Pas encore d'évaluation
- Pulmonary Function TestDocument9 pagesPulmonary Function TestMarivic DianoPas encore d'évaluation
- 13th & 14th WK - Oxygen Therapy With VideoDocument89 pages13th & 14th WK - Oxygen Therapy With VideoJesus Mario Lopez100% (1)
- Nursing Care Plan For HypoglycemiaDocument3 pagesNursing Care Plan For HypoglycemiaPuteri AzmanPas encore d'évaluation
- Standing Order-Diarrhea DraftDocument1 pageStanding Order-Diarrhea DraftKatelyn Brissey50% (2)
- Nursing Management of Patient With Mechanical VentilationDocument77 pagesNursing Management of Patient With Mechanical Ventilationrojina poudel0% (1)
- Team NursingDocument4 pagesTeam Nursingsagami.g80% (5)
- Nursing Care of The Child Undergoing A TonsillectomyDocument2 pagesNursing Care of The Child Undergoing A Tonsillectomykelsey0% (1)
- NCP For MGDocument1 pageNCP For MGSandra MedinaPas encore d'évaluation
- Nursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisDocument17 pagesNursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisJordz Placi100% (1)
- MI Chest Pain AssessmentDocument5 pagesMI Chest Pain AssessmentDharline Abbygale Garvida AgullanaPas encore d'évaluation
- Role Av Aids in Clinical TeachingDocument16 pagesRole Av Aids in Clinical Teachingtankmp100% (1)
- Cva NCP AnxietyDocument1 pageCva NCP AnxietyQueenElsaDeVeraPas encore d'évaluation
- Assessing and Managing Risk of AspirationDocument6 pagesAssessing and Managing Risk of AspirationaianrPas encore d'évaluation
- NCP LocDocument2 pagesNCP LocMel RodolfoPas encore d'évaluation
- Nursing Care PlanDocument4 pagesNursing Care PlanAdreanah Martin RañisesPas encore d'évaluation
- Nursing Care Plan: Risk For Disuse SyndromeDocument2 pagesNursing Care Plan: Risk For Disuse SyndromeRozsy FakhrurPas encore d'évaluation
- Angina Pectoris Nursing Care PlanDocument1 pageAngina Pectoris Nursing Care PlanjamieboyRN86% (7)
- For NCP PipsDocument9 pagesFor NCP PipsJulius BucoyPas encore d'évaluation
- NCP-Case Presentation (CHF)Document4 pagesNCP-Case Presentation (CHF)Jessamine EnriquezPas encore d'évaluation
- What Are The Signs and Symptoms of Heart Failure?Document4 pagesWhat Are The Signs and Symptoms of Heart Failure?Lara TechiesPas encore d'évaluation
- Nursing Interventions CHFDocument3 pagesNursing Interventions CHFbanyenye25100% (1)
- NCP for AGE Deficient Fluid VolumeDocument2 pagesNCP for AGE Deficient Fluid VolumekarenbelnasPas encore d'évaluation
- Heart Failure Care PlanDocument5 pagesHeart Failure Care PlanJustin StuartPas encore d'évaluation
- Nursing InterventionsDocument2 pagesNursing InterventionsJanine Paola CabangilPas encore d'évaluation
- Reduced Cardiac Output CareDocument4 pagesReduced Cardiac Output CarePaul PraveenPas encore d'évaluation
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanPas encore d'évaluation
- NCPDocument15 pagesNCPCamille PinedaPas encore d'évaluation
- Nursing Care Plans for Diarrhea, Dehydration & Acute PainDocument13 pagesNursing Care Plans for Diarrhea, Dehydration & Acute PainRocel DevillesPas encore d'évaluation
- Detecting Increased Intracranial Pressure in a 6-Year-Old with Head InjuryDocument7 pagesDetecting Increased Intracranial Pressure in a 6-Year-Old with Head InjuryAuni Akif Aleesa100% (1)
- Febrile FitDocument3 pagesFebrile FitAuni Akif AleesaPas encore d'évaluation
- Table 1 of TMC501 Lesson 2 Kampung Life (Prepared by Dr. Neo Kian Sen)Document2 pagesTable 1 of TMC501 Lesson 2 Kampung Life (Prepared by Dr. Neo Kian Sen)Auni Akif AleesaPas encore d'évaluation
- MDG Children and Adolescents SummaryDocument74 pagesMDG Children and Adolescents SummaryMohd Saufee50% (2)
- Grammar MandarinDocument1 pageGrammar MandarinAuni Akif AleesaPas encore d'évaluation
- CakeDocument1 pageCakeAuni Akif AleesaPas encore d'évaluation
- Questions and Answers SessionDocument1 pageQuestions and Answers SessionAuni Akif AleesaPas encore d'évaluation
- Congenital Heart Disease - ASDDocument36 pagesCongenital Heart Disease - ASDAuni Akif AleesaPas encore d'évaluation
- Grammar MandarinDocument1 pageGrammar MandarinAuni Akif AleesaPas encore d'évaluation
- Table 2 of TMC501 Lesson 3 Go On Holiday (Prepared by Dr. Neo Kian Sen)Document4 pagesTable 2 of TMC501 Lesson 3 Go On Holiday (Prepared by Dr. Neo Kian Sen)Auni Akif AleesaPas encore d'évaluation
- CandyDocument1 pageCandyAuni Akif AleesaPas encore d'évaluation
- Cell, TissueDocument8 pagesCell, TissueAuni Akif AleesaPas encore d'évaluation
- CandyDocument1 pageCandyAuni Akif AleesaPas encore d'évaluation
- CheeseDocument1 pageCheeseAuni Akif AleesaPas encore d'évaluation
- ShipsDocument1 pageShipsAuni Akif AleesaPas encore d'évaluation
- CakeDocument1 pageCakeAuni Akif AleesaPas encore d'évaluation
- LadderDocument1 pageLadderAuni Akif AleesaPas encore d'évaluation
- BalloonDocument1 pageBalloonAuni Akif AleesaPas encore d'évaluation
- RainDocument1 pageRainAuni Akif Aleesa50% (2)
- KitesDocument1 pageKitesAuni Akif AleesaPas encore d'évaluation
- FrogDocument1 pageFrogAuni Akif AleesaPas encore d'évaluation
- TrainDocument1 pageTrainAuni Akif AleesaPas encore d'évaluation
- VSD Guide: Types, Causes and Nursing Care for Ventricular Septal DefectDocument53 pagesVSD Guide: Types, Causes and Nursing Care for Ventricular Septal DefectAuni Akif AleesaPas encore d'évaluation
- JellyfishDocument1 pageJellyfishAuni Akif AleesaPas encore d'évaluation
- Congenital Heart Disease - ASDDocument36 pagesCongenital Heart Disease - ASDAuni Akif Aleesa100% (1)
- Quick NOteDocument7 pagesQuick NOteAuni Akif Aleesa100% (1)
- Cell, TissueDocument8 pagesCell, TissueAuni Akif AleesaPas encore d'évaluation
- Weight Management and Body Shaping System 90: Transform Your Life in DaysDocument6 pagesWeight Management and Body Shaping System 90: Transform Your Life in DaysZesika N. AnnisaPas encore d'évaluation
- MONOSACCHARIDEDocument2 pagesMONOSACCHARIDEPRINTDESK by Dan100% (1)
- Kellogs Case StudyDocument28 pagesKellogs Case StudyVikas RajputPas encore d'évaluation
- 10-11 - Anti-Hyperlipidemic Drugs (Summary SAQ and MCQS)Document6 pages10-11 - Anti-Hyperlipidemic Drugs (Summary SAQ and MCQS)Purvak MahajanPas encore d'évaluation
- Carbohydrate: N) - However, Not All Carbohydrates Conform To ThisDocument13 pagesCarbohydrate: N) - However, Not All Carbohydrates Conform To ThisCrow LordPas encore d'évaluation
- Lisa Dorfman - The Vegetarian Sports Nutrition Guide - Peak Performance For Everyone From Beginners To Gold Medalists (1999, Wiley)Document279 pagesLisa Dorfman - The Vegetarian Sports Nutrition Guide - Peak Performance For Everyone From Beginners To Gold Medalists (1999, Wiley)Gustavo HerzPas encore d'évaluation
- Thanda Matlab..................Document33 pagesThanda Matlab..................Upnishad MishraPas encore d'évaluation
- Analysis of The Official Resolution To Implement The IEPS Tax, To Sugar BeveragesDocument2 pagesAnalysis of The Official Resolution To Implement The IEPS Tax, To Sugar BeveragesMariel LunaPas encore d'évaluation
- 1129 - Health and Wellbeing - tcm143-663582Document4 pages1129 - Health and Wellbeing - tcm143-663582Eugen CrivceanschiPas encore d'évaluation
- The Zero Carb DietDocument69 pagesThe Zero Carb DietJivoPas encore d'évaluation
- Dietetics Module: Therapeutic Diets and Chronic Disease ManagementDocument24 pagesDietetics Module: Therapeutic Diets and Chronic Disease ManagementSara MagedPas encore d'évaluation
- Kesihatan & Kesegahteraan Melalui Sains MandianDocument40 pagesKesihatan & Kesegahteraan Melalui Sains Mandianosha911Pas encore d'évaluation
- Managing Nutrition for a Diabetic Patient with PneumoniaDocument5 pagesManaging Nutrition for a Diabetic Patient with PneumoniaCazze SunioPas encore d'évaluation
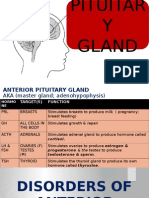
- Disorders of Pituitary GlandDocument34 pagesDisorders of Pituitary GlandninaaltheaPas encore d'évaluation
- Supersize Me: An Exploratory Analysis of The Nutritional Content in Mcdonald's Menu ItemsDocument7 pagesSupersize Me: An Exploratory Analysis of The Nutritional Content in Mcdonald's Menu ItemsIjahss JournalPas encore d'évaluation
- SetyaningrumrahmawatyDocument3 pagesSetyaningrumrahmawatyBoh Cucu KaraengPas encore d'évaluation
- Ben Johnson's Weight Training Program by Coach Charlie FrancisDocument7 pagesBen Johnson's Weight Training Program by Coach Charlie Francismichal900_40834675350% (2)
- Assessment of Body Image Flexibility - BIAAQDocument11 pagesAssessment of Body Image Flexibility - BIAAQomsohamomPas encore d'évaluation
- Family Health ManagementDocument12 pagesFamily Health ManagementVincent CuyucaPas encore d'évaluation
- Benefits of TriphalaDocument4 pagesBenefits of TriphalaAditya Sharma100% (1)
- Physical Education and Health Grade 11 Quiz AnswersDocument12 pagesPhysical Education and Health Grade 11 Quiz AnswersColeen ColladoPas encore d'évaluation
- Apovian 2016Document10 pagesApovian 2016Sandy PranadaPas encore d'évaluation
- Foaming Capacity of Soaps Investigatory Projects Chemistry Class 12 CbseDocument17 pagesFoaming Capacity of Soaps Investigatory Projects Chemistry Class 12 CbseChandan Kumar SharmaPas encore d'évaluation
- Full-Sentence Speech FinalDocument2 pagesFull-Sentence Speech Finalapi-363883917Pas encore d'évaluation
- Stability Ball Progressions: Athletic CompanyDocument8 pagesStability Ball Progressions: Athletic CompanymcgowenkPas encore d'évaluation
- PG 9-2Document1 pagePG 9-2Consetta GottmanPas encore d'évaluation
- Dr. Ika Prasetya Wijaya SPPD-KKV, Finasim: Samarinda: 5 Januari 1968Document29 pagesDr. Ika Prasetya Wijaya SPPD-KKV, Finasim: Samarinda: 5 Januari 1968SriNoviantiPas encore d'évaluation
- According To The Study of Len KravitzDocument4 pagesAccording To The Study of Len KravitzRon NecesitoPas encore d'évaluation
- Nutrition for the Community Exam QuestionsDocument6 pagesNutrition for the Community Exam QuestionsRamBabuMeenaPas encore d'évaluation
- Chapter 04Document17 pagesChapter 04Ena BorlatPas encore d'évaluation