Vous aimerez peut-être aussi
- Iccc Xi Carcinomas and Other Malignant Epithelial Neoplasms: IncidenceDocument10 pagesIccc Xi Carcinomas and Other Malignant Epithelial Neoplasms: Incidencewawansiswadi01Pas encore d'évaluation
- Epidemiology Vit A Def 2009Document40 pagesEpidemiology Vit A Def 2009Dessy Yusra ZahiraPas encore d'évaluation
- Complications of Cardiopulmonary Resuscitation: Original Research - Orijinal AraştırmaDocument8 pagesComplications of Cardiopulmonary Resuscitation: Original Research - Orijinal AraştırmaTatanPas encore d'évaluation
- Male/Female Ratio:: Spindle Cell Lipomatous LesionsDocument10 pagesMale/Female Ratio:: Spindle Cell Lipomatous LesionsMuhammad ZainPas encore d'évaluation
- 4 Methods of Data Organizing and PresentationDocument47 pages4 Methods of Data Organizing and Presentationeshet chafPas encore d'évaluation
- Cases Surgery For Non-Melanoma Skin Cancers: bcc, scc, mcc.D'EverandCases Surgery For Non-Melanoma Skin Cancers: bcc, scc, mcc.Pas encore d'évaluation
- BAB IV Translate ArifDocument11 pagesBAB IV Translate ArifDoc Arif AkhmadPas encore d'évaluation
- Biostatistics Lecture - 1 - IntroductionDocument36 pagesBiostatistics Lecture - 1 - IntroductionDr. Mahmoud Abbas Mahmoud Al-Naimi50% (4)
- Thyroid Cancer in Young Adults: Anita K. Ying, Winston Huh, Sarah Bottomley, Douglas B. Evans, and Steven G. WaguespackDocument17 pagesThyroid Cancer in Young Adults: Anita K. Ying, Winston Huh, Sarah Bottomley, Douglas B. Evans, and Steven G. WaguespackBenny KurniawanPas encore d'évaluation
- Obesity: Issues and Challenges: With Particular Reference To Adult Malaysian)Document65 pagesObesity: Issues and Challenges: With Particular Reference To Adult Malaysian)mrashidi_9Pas encore d'évaluation
- Spector 2015Document15 pagesSpector 2015KAREN JAZMIN RUIZ MONROYPas encore d'évaluation
- s41598 018 35903 5Document9 pagess41598 018 35903 5leartaPas encore d'évaluation
- Classification of Thyroid CarcinomaDocument26 pagesClassification of Thyroid CarcinomaSifu Perniagaan MayaPas encore d'évaluation
- Management of Rhabdomyosarco MA: Presenter: DR Manas Dubey Moderator: DR Rakesh DhankharDocument64 pagesManagement of Rhabdomyosarco MA: Presenter: DR Manas Dubey Moderator: DR Rakesh DhankharRebuma MegersaPas encore d'évaluation
- The Prevalence of Symptoms and Signs of Temporomandibular Disorders Among A Group of Young Adult Jordanian PopulationDocument7 pagesThe Prevalence of Symptoms and Signs of Temporomandibular Disorders Among A Group of Young Adult Jordanian PopulationMuhammad Iqwan MHPas encore d'évaluation
- Soluk Tekkesin2020Document6 pagesSoluk Tekkesin2020ay lmaoPas encore d'évaluation
- Incidence and Treatment of Complications in PatientsDocument6 pagesIncidence and Treatment of Complications in Patientszfadhli.s.96Pas encore d'évaluation
- Introduction To BiostatisticsDocument31 pagesIntroduction To BiostatisticsNourhan KhattabPas encore d'évaluation
- Pediatric and Adult ECMO TalkDocument58 pagesPediatric and Adult ECMO TalkPERFUZIJAPas encore d'évaluation
- 03 - SÀNG LOC QUÝ 2 (Tiếng Anh)Document48 pages03 - SÀNG LOC QUÝ 2 (Tiếng Anh)huyentruonghmPas encore d'évaluation
- Descriptive Statistics (31-1) BiostatisticsDocument40 pagesDescriptive Statistics (31-1) BiostatisticsBlackstarPas encore d'évaluation
- WK 1b BiostatDocument38 pagesWK 1b BiostatRaizane Sky PalecPas encore d'évaluation
- Bechat (5), Andrews (6) and Others: Printed N U.S.ADocument4 pagesBechat (5), Andrews (6) and Others: Printed N U.S.AAldhy D'souljaPas encore d'évaluation
- 8th Edition of The AJCC - TNM Staging System of Thyroid Cancer - What To Expect (ITCO#2)Document5 pages8th Edition of The AJCC - TNM Staging System of Thyroid Cancer - What To Expect (ITCO#2)Valentina IndahPas encore d'évaluation
- Clinico-Mycological Evaluation of Dermatophytes in Superficial Fungal Infections in A Tertiary Care Centre, West Uttar PradeshDocument8 pagesClinico-Mycological Evaluation of Dermatophytes in Superficial Fungal Infections in A Tertiary Care Centre, West Uttar Pradeshindex PubPas encore d'évaluation
- Epidemiology of Venous Thromboembolic DiseaseDocument5 pagesEpidemiology of Venous Thromboembolic DiseaseVirginia WongPas encore d'évaluation
- Epidemiology and The Health Transition: Neglected Chronic Diseases (NCD) in AdultsDocument21 pagesEpidemiology and The Health Transition: Neglected Chronic Diseases (NCD) in AdultsBhagiaswari KodapallyPas encore d'évaluation
- Prof. Dr. Dr. Hinky Hindra Irawan Satari, Sp.A (K), M.TropPaed - The Role of Pneumococcal Conjugate Vaccines (PCVS) in InfantsDocument38 pagesProf. Dr. Dr. Hinky Hindra Irawan Satari, Sp.A (K), M.TropPaed - The Role of Pneumococcal Conjugate Vaccines (PCVS) in InfantsJayantiPas encore d'évaluation
- Human Papillomavirus (HPV) : The DiseaseDocument19 pagesHuman Papillomavirus (HPV) : The Diseasecoffee.and.tvPas encore d'évaluation
- I. Primary 1. Epithelial 2. Non-EpithelialDocument25 pagesI. Primary 1. Epithelial 2. Non-EpithelialSifu Perniagaan MayaPas encore d'évaluation
- Pediatric OncologyDocument265 pagesPediatric OncologyTewodros GetahunPas encore d'évaluation
- Etiopathogenesis & Staging of Cancer BreastDocument25 pagesEtiopathogenesis & Staging of Cancer Breastapi-3701915Pas encore d'évaluation
- Creighton University School of Medicine Department of Pathology MDDocument36 pagesCreighton University School of Medicine Department of Pathology MDDeba P SarmaPas encore d'évaluation
- Melanocytes, Mole, MelanomaDocument35 pagesMelanocytes, Mole, MelanomaDeba P SarmaPas encore d'évaluation
- Sacrococcygeal Teratoma A Tumor at The Center of EmbryogenesisDocument8 pagesSacrococcygeal Teratoma A Tumor at The Center of EmbryogenesisLuis Ruelas SanchezPas encore d'évaluation
- 6 Spatz 1 Paris Melanoma 042618Document29 pages6 Spatz 1 Paris Melanoma 042618sviatohaPas encore d'évaluation
- Review of Cystic and Solid TumorDocument6 pagesReview of Cystic and Solid TumorAnonymous syRbQm6Pas encore d'évaluation
- Angelic - Doc - Breast CancerDocument12 pagesAngelic - Doc - Breast CancerAngy100% (2)
- Grading Prognosis MeningiomaDocument7 pagesGrading Prognosis MeningiomaChiki CacaPas encore d'évaluation
- Lung Cancer: I Gede Ketut SajinadiyasaDocument81 pagesLung Cancer: I Gede Ketut Sajinadiyasadr.Dewi Shintaher100% (1)
- Chest X-Ray Findings of Pulmonary Tuberculosis With Diabetes MellitusDocument4 pagesChest X-Ray Findings of Pulmonary Tuberculosis With Diabetes MellitusRohitPas encore d'évaluation
- A Comprehensive Review of Risk Factors For Venous Thromboembolism - From Epidemiology To PathophysiologyDocument24 pagesA Comprehensive Review of Risk Factors For Venous Thromboembolism - From Epidemiology To Pathophysiologyirvanardian94Pas encore d'évaluation
- Smoking CessationDocument89 pagesSmoking Cessationenjagan67% (3)
- Campbell-Walsh Urology, 12th Edition 1Document21 pagesCampbell-Walsh Urology, 12th Edition 1NICOLE CARPIO MALAGAPas encore d'évaluation
- Dermatopathology: Melanocytes, Mole And. Melanoma 2008 Pathology Grand Round at CUMCDocument35 pagesDermatopathology: Melanocytes, Mole And. Melanoma 2008 Pathology Grand Round at CUMCDeba P SarmaPas encore d'évaluation
- Articles: BackgroundDocument9 pagesArticles: Backgroundalchemistbro 007Pas encore d'évaluation
- Brain Sciences: Acute Regression in Young People With Down SyndromeDocument9 pagesBrain Sciences: Acute Regression in Young People With Down SyndromePar DoPas encore d'évaluation
- Nejmra 1514010Document12 pagesNejmra 1514010Vanessa Alvarenga BezerraPas encore d'évaluation
- 27.2 Nikfarjam 11-18Document8 pages27.2 Nikfarjam 11-18afm26Pas encore d'évaluation
- Laryngeal Cancer, Risk Factors, Symptoms and Treatment PDFDocument8 pagesLaryngeal Cancer, Risk Factors, Symptoms and Treatment PDFandre halimPas encore d'évaluation
- Reti No Blast OmaDocument6 pagesReti No Blast OmaFebyWulansariPas encore d'évaluation
- Lecture 27.2. Male Genital Tumors (Testis - Penile Cancer)Document51 pagesLecture 27.2. Male Genital Tumors (Testis - Penile Cancer)krisnadewirahadiPas encore d'évaluation
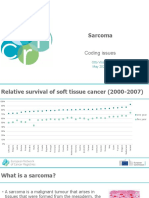
- ENCR2021 S4 SarcomaDocument28 pagesENCR2021 S4 SarcomaFernando SilalahiPas encore d'évaluation
- CT SS (Chest Computed Tomography Severity Score)Document2 pagesCT SS (Chest Computed Tomography Severity Score)Fathur RahmanPas encore d'évaluation
- Critical Reviews in Oncology / HematologyDocument11 pagesCritical Reviews in Oncology / HematologyAhmad aPas encore d'évaluation
- Rafki Hidayat, Kamal Basri Siregar, SuyatnoDocument8 pagesRafki Hidayat, Kamal Basri Siregar, SuyatnoWahyu IndraPas encore d'évaluation
- Magnitude and Trends of Noncommunicable DiseasesDocument21 pagesMagnitude and Trends of Noncommunicable DiseasesCandra BumiPas encore d'évaluation
- SC 2009118Document5 pagesSC 2009118Yanne LewerissaPas encore d'évaluation
- LP Tumor SinonasalDocument26 pagesLP Tumor SinonasalLydia Citra DewiPas encore d'évaluation
- Thesis Brand BlanketDocument4 pagesThesis Brand BlanketKayla Smith100% (2)
- Pediatric Gynecology BaruDocument79 pagesPediatric Gynecology BaruJosephine Irena100% (2)
- Inverse Curve Trip Time Calculation: Enter Values in White CellDocument3 pagesInverse Curve Trip Time Calculation: Enter Values in White CellVijay FxPas encore d'évaluation
- Lesson Notes Lecture 14Document5 pagesLesson Notes Lecture 14Quantum SaudiPas encore d'évaluation
- Excretory Products and Their EliminationDocument13 pagesExcretory Products and Their Eliminationaravind kishanPas encore d'évaluation
- T 1246784488 17108574 Street Lighting Control Based On LonWorks Power Line CommunicationDocument3 pagesT 1246784488 17108574 Street Lighting Control Based On LonWorks Power Line CommunicationsryogaaPas encore d'évaluation
- FP Lecture Midterm Exam Sec - Sem.2020Document4 pagesFP Lecture Midterm Exam Sec - Sem.2020SAEEDA ALMUQAHWIPas encore d'évaluation
- EndressHauser HART CommunicatorDocument1 pageEndressHauser HART CommunicatorGhafur AgusPas encore d'évaluation
- Chemical Process DebottleneckingDocument46 pagesChemical Process DebottleneckingAhmed Ansari100% (2)
- Practical Considerations in Modeling: Physical Interactions Taking Place Within A BodyDocument35 pagesPractical Considerations in Modeling: Physical Interactions Taking Place Within A BodyFábio1 GamaPas encore d'évaluation
- 02-09-18 SR - IZ Jee-Adv 2011-P1 PTA-03 Q PDFDocument31 pages02-09-18 SR - IZ Jee-Adv 2011-P1 PTA-03 Q PDFswarupPas encore d'évaluation
- Psalm151 160Document3 pagesPsalm151 160Gina KristenPas encore d'évaluation
- UntitledDocument413 pagesUntitledjgj38j90Pas encore d'évaluation
- 65 ActsDocument178 pages65 ActsComprachosPas encore d'évaluation
- Etl 213-1208.10 enDocument1 pageEtl 213-1208.10 enhossamPas encore d'évaluation
- The Moon That Embrace The SunDocument36 pagesThe Moon That Embrace The SunNorma PuspitaPas encore d'évaluation
- 1704 Broschuere Metal-Coating en EinzelseitenDocument8 pages1704 Broschuere Metal-Coating en EinzelseiteninterponPas encore d'évaluation
- DUPIXENT Doctor Discussion GuideDocument4 pagesDUPIXENT Doctor Discussion GuideTAP THANH CHAUPas encore d'évaluation
- Joseph Conrad - Heart of DarknessDocument86 pagesJoseph Conrad - Heart of DarknessCaztor SscPas encore d'évaluation
- Chapter 5, Abdominal TraumaDocument41 pagesChapter 5, Abdominal TraumaRandy HarrisPas encore d'évaluation
- Faithgirlz Handbook, Updated and ExpandedDocument15 pagesFaithgirlz Handbook, Updated and ExpandedFaithgirlz75% (4)
- Practical - 2: Preparation of The FixativeDocument14 pagesPractical - 2: Preparation of The FixativeIseth ISethPas encore d'évaluation
- DLL - Mapeh 6 - Q2 - W8Document6 pagesDLL - Mapeh 6 - Q2 - W8Joe Marie FloresPas encore d'évaluation
- 1943 Dentures Consent FormDocument2 pages1943 Dentures Consent FormJitender ReddyPas encore d'évaluation
- Design of Cycle Rickshaw For School ChildrenDocument23 pagesDesign of Cycle Rickshaw For School ChildrenAditya GuptaPas encore d'évaluation
- Science7 q2 Mod6of8 Asexual Sexualrep v2Document26 pagesScience7 q2 Mod6of8 Asexual Sexualrep v2Ishi OcheaPas encore d'évaluation
- Feasibility Study On The Seaweed Kappaphycus Alvarezii Cultivation Site in Indari Waters ofDocument9 pagesFeasibility Study On The Seaweed Kappaphycus Alvarezii Cultivation Site in Indari Waters ofUsman MadubunPas encore d'évaluation
- Anchor Chart-Describing Words-Descriptive Details of Setting and Character PDFDocument2 pagesAnchor Chart-Describing Words-Descriptive Details of Setting and Character PDFdellindiaPas encore d'évaluation
- MSDS PaintingDocument81 pagesMSDS PaintingPaulina PaskahriaPas encore d'évaluation
- SweetenersDocument23 pagesSweetenersNur AfifahPas encore d'évaluation