Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- CISCO Router Software - Configuration PDFDocument408 pagesCISCO Router Software - Configuration PDFasalihovicPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Fundamentals of Physics Sixth Edition: Halliday Resnick WalkerDocument4 pagesFundamentals of Physics Sixth Edition: Halliday Resnick WalkerAhmar KhanPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Robot Sensors and TransducersDocument176 pagesRobot Sensors and TransducerssakthivelPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Presentation: Isa Test Sets Training Course - 2014Document5 pagesPresentation: Isa Test Sets Training Course - 2014Sultan Uddin KhanPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- International Marketing-Assignment No. 01Document36 pagesInternational Marketing-Assignment No. 01Faisal Shahzad60% (5)
- PLX7100A Digital Mobile C-Arm X-Ray Machine: 1. Technical SpecificationDocument3 pagesPLX7100A Digital Mobile C-Arm X-Ray Machine: 1. Technical SpecificationAbdalhakeem AlturkyPas encore d'évaluation
- Creative Computing v06 n12 1980 DecemberDocument232 pagesCreative Computing v06 n12 1980 Decemberdarkstar314Pas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Triosonate in F (TWV 42-F7)Document17 pagesTriosonate in F (TWV 42-F7)EDMILSON BRUNO DO NASCIMENTOPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- GB-T 5137.1-2002 Test Methods of Safety Glazing Materials Used On Road Vehicles Part1 Mechanical Properties TestsDocument14 pagesGB-T 5137.1-2002 Test Methods of Safety Glazing Materials Used On Road Vehicles Part1 Mechanical Properties TestsRandyzhuPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Origin and Structure of The EarthDocument8 pagesOrigin and Structure of The EarthRobin Suarez ViladoPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Numerical ModelDocument61 pagesNumerical ModelAlbert AguileraPas encore d'évaluation
- Demag KBK Alu Enclosed Track SystemDocument2 pagesDemag KBK Alu Enclosed Track SystemMAGSTPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
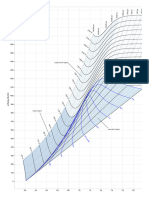
- Mollier Enthalpy Entropy Chart For Steam - US UnitsDocument1 pageMollier Enthalpy Entropy Chart For Steam - US Unitslin tongPas encore d'évaluation
- Oracle Goldengate: Oracle Installation and Setup Guide 11 Release 2 (11.2.1.0.0)Document188 pagesOracle Goldengate: Oracle Installation and Setup Guide 11 Release 2 (11.2.1.0.0)kashifmeoPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Magnetophoresis and Electromagnetophoresis of Microparticles in LiquidsDocument7 pagesMagnetophoresis and Electromagnetophoresis of Microparticles in Liquids3issazakaPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Psychometric Development and Validation of GaslightingDocument15 pagesPsychometric Development and Validation of GaslightingYang ZhangPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Sample Paper III (Science) - Question PaperDocument21 pagesSample Paper III (Science) - Question Paperfathima MiranPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- SC431 Lecture No. 4 Economic Comparisons (Continued)Document51 pagesSC431 Lecture No. 4 Economic Comparisons (Continued)Joseph BaruhiyePas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- 15Document20 pages15Allen Rey YeclaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Kemetic Tree of LifeDocument1 pageThe Kemetic Tree of LifeFlorin CiudinPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Newvhdl Syllabus (It&Cse)Document2 pagesNewvhdl Syllabus (It&Cse)Mude Kishore NaikPas encore d'évaluation
- 1922 A Textbook of Balochi LanguageDocument228 pages1922 A Textbook of Balochi LanguageAnonymous 0ywnNS29EGPas encore d'évaluation
- PR100 BrochureDocument28 pagesPR100 Brochuregus289Pas encore d'évaluation
- LAAMS Technical Summary Tensar+Document17 pagesLAAMS Technical Summary Tensar+Janaki RamPas encore d'évaluation
- 2.data Types Ver2Document56 pages2.data Types Ver2qwernasdPas encore d'évaluation
- C V RamanDocument8 pagesC V RamanJayesh KomalwarPas encore d'évaluation
- ImmunologyDocument8 pagesImmunologyማላያላም ማላያላም89% (9)
- Template Question BankDocument11 pagesTemplate Question Bankeshwar_worldPas encore d'évaluation
- API ISCAN-LITE ScannerDocument4 pagesAPI ISCAN-LITE Scannergrg_grePas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Bent's RuleDocument3 pagesBent's RuleEdwinPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)