Vous aimerez peut-être aussi
- MS BulletsDocument66 pagesMS BulletsMox SwanPas encore d'évaluation
- Prescription Template 07Document2 pagesPrescription Template 07vincent100% (1)
- Vom Otc PDFDocument4 pagesVom Otc PDFAnonymous 45z6m4eE7pPas encore d'évaluation
- Enumerate The FollowingDocument1 pageEnumerate The FollowingAnna Marie Carmen Cervantes100% (1)
- GHB FactsheetDocument2 pagesGHB FactsheetABC Action NewsPas encore d'évaluation
- VOCSN Prescription TemplateDocument2 pagesVOCSN Prescription TemplateDZADZA YAOVIPas encore d'évaluation
- I Found This Extremely Interesting and Have Created It As A PDFDocument10 pagesI Found This Extremely Interesting and Have Created It As A PDFkatiesomervillePas encore d'évaluation
- Cardio-Pulmo Discharge SummaryDocument2 pagesCardio-Pulmo Discharge SummaryIndranil SinhaPas encore d'évaluation
- Checkra 1 NDocument1 pageCheckra 1 NVioPas encore d'évaluation
- UE3 Auto Report Ini Dump 0001Document374 pagesUE3 Auto Report Ini Dump 0001Grant DePoyPas encore d'évaluation
- Evil Mass Storage - DriverEntry - Article by Daniel BrooksDocument13 pagesEvil Mass Storage - DriverEntry - Article by Daniel BrooksWeronika WyszynskaPas encore d'évaluation
- SS7 Whitepaper Ver 1.41Document19 pagesSS7 Whitepaper Ver 1.41Anonymous Ie0oEXP2ePas encore d'évaluation
- Smart CardDocument14 pagesSmart CardPraveen KumarPas encore d'évaluation
- Controlled Substances ListDocument11 pagesControlled Substances ListNickPas encore d'évaluation
- StatsLists01 12 12Document95 pagesStatsLists01 12 12sadim22Pas encore d'évaluation
- Platinum Transaction Program GuideDocument47 pagesPlatinum Transaction Program GuideSSGFL10% (1)
- Toy Mountain Drop Off Locations 2021Document1 pageToy Mountain Drop Off Locations 2021CTV OttawaPas encore d'évaluation
- Card Business Debit and Credit CardsDocument17 pagesCard Business Debit and Credit CardsmahiPas encore d'évaluation
- Indica CBD Vape Carts SmackdownuqontDocument2 pagesIndica CBD Vape Carts Smackdownuqontpaulbat11Pas encore d'évaluation
- Answer Key For NCLEX® Style Questions in Text: Elkin: Nursing Interventions and Clinical Skills, 4 EditionDocument6 pagesAnswer Key For NCLEX® Style Questions in Text: Elkin: Nursing Interventions and Clinical Skills, 4 EditionSilvia FierroPas encore d'évaluation
- Thief Economic CrimeDocument17 pagesThief Economic CrimeMatt LocardPas encore d'évaluation
- Walmart Drug ListDocument6 pagesWalmart Drug ListShirley Pigott MDPas encore d'évaluation
- Processing PrescriptionsDocument24 pagesProcessing PrescriptionsChrissiePas encore d'évaluation
- ATI Assignment # 6Document9 pagesATI Assignment # 6Tee Wood0% (2)
- Instructions: After Visit SummaryDocument10 pagesInstructions: After Visit SummaryKelly Arington McgrealPas encore d'évaluation
- HHS Provider Relief Fund FY22Document56 pagesHHS Provider Relief Fund FY22Ivan HerreraPas encore d'évaluation
- FentanylDocument2 pagesFentanylAdrianne Bazo100% (1)
- The Lazarus Constellation A Study On North Korean Malware 1584232708Document64 pagesThe Lazarus Constellation A Study On North Korean Malware 1584232708Pablo AvilesPas encore d'évaluation
- Spice (PDF) - 201504161325508316 PDFDocument30 pagesSpice (PDF) - 201504161325508316 PDFMartin KissPas encore d'évaluation
- Jim's LawncareDocument18 pagesJim's LawncareJakeDickersonPas encore d'évaluation
- 80096503-001-E ID TECH SecureMag OPOS User's ManualDocument34 pages80096503-001-E ID TECH SecureMag OPOS User's ManualEvangelista Francisco LacombaPas encore d'évaluation
- Galileo RCS - Installing The Entire Espionage Platform - Hyperion BristolDocument7 pagesGalileo RCS - Installing The Entire Espionage Platform - Hyperion BristolAli Asad SahuPas encore d'évaluation
- Create Login Application in Excel Macro Using Visual Basic: Karthikeyan K ArticleDocument16 pagesCreate Login Application in Excel Macro Using Visual Basic: Karthikeyan K Articlefranklaer-2Pas encore d'évaluation
- PrescriptionDocument18 pagesPrescriptionAlphahin 17Pas encore d'évaluation
- 156 - A - Further Information RECIPEDocument6 pages156 - A - Further Information RECIPEKeith userPas encore d'évaluation
- CSP ReportDocument9 pagesCSP ReportS ZPas encore d'évaluation
- DU D Unit Question Bank 2018-19Document4 pagesDU D Unit Question Bank 2018-19Rajin Mahmud KhanPas encore d'évaluation
- Alcohol Addiction Research From Animal Models To ClinicsDocument12 pagesAlcohol Addiction Research From Animal Models To ClinicsJef_8Pas encore d'évaluation
- 10 Kinds of Drug AbuseDocument10 pages10 Kinds of Drug AbuseJennifer Piloton CañetePas encore d'évaluation
- BDM Letter of AuthorityDocument2 pagesBDM Letter of Authoritybobby1line100% (1)
- Simple Low Cost UHF RFID Reader: Pavel V. Nikitin, Shashi Ramamurthy, Rene MartinezDocument2 pagesSimple Low Cost UHF RFID Reader: Pavel V. Nikitin, Shashi Ramamurthy, Rene MartinezHuỳnh Thanh DưPas encore d'évaluation
- Sb5100 Modification TutorialDocument4 pagesSb5100 Modification TutorialoptimusmaximusyPas encore d'évaluation
- Basics of TCP/IP, Switching, Routing and Firewalling.: WWW - Google.deDocument17 pagesBasics of TCP/IP, Switching, Routing and Firewalling.: WWW - Google.deeva sharmaPas encore d'évaluation
- Professional Reference List CDocument1 pageProfessional Reference List Capi-488492498Pas encore d'évaluation
- Codeine From WikipediaDocument12 pagesCodeine From WikipediaMuhammad Miftahul HudaPas encore d'évaluation
- NavyDocument1 659 pagesNavygorgon34Pas encore d'évaluation
- Android EmulatorDocument23 pagesAndroid EmulatorKim De Castro MalagdayPas encore d'évaluation
- ATM Case Study, Part 1: Object-Oriented Design With The UMLDocument46 pagesATM Case Study, Part 1: Object-Oriented Design With The UMLVaidehiBaporikarPas encore d'évaluation
- Security Awareness: The Dangers of Using ATM How To Protect Yourself?Document61 pagesSecurity Awareness: The Dangers of Using ATM How To Protect Yourself?chandru_aspPas encore d'évaluation
- Presented By: Niraj AryalDocument5 pagesPresented By: Niraj AryalNeeraj AryalPas encore d'évaluation
- EMV Transactions With Universal SDKDocument27 pagesEMV Transactions With Universal SDKTebogo Mmaswi MakhubelaPas encore d'évaluation
- Sars-Cov-2 (Covid-19) : Patient Specimen PhysicianDocument1 pageSars-Cov-2 (Covid-19) : Patient Specimen PhysicianBrayan AtiroPas encore d'évaluation
- Pos Machine Security TestingDocument6 pagesPos Machine Security TestingAnkit DPas encore d'évaluation
- How To Outsmart Your Smart MeterDocument28 pagesHow To Outsmart Your Smart MeterAlienUFOPas encore d'évaluation
- Sustainable Chemistry and Pharmacy: Rocío L. Pérez, Graciela M. EscandarDocument12 pagesSustainable Chemistry and Pharmacy: Rocío L. Pérez, Graciela M. EscandarGeorgiana-LuizaPas encore d'évaluation
- UNIT 4 - Computer Crime: Omputer Heft Nauthorised SE Ccess Odification HE Omputer Isuse CTDocument9 pagesUNIT 4 - Computer Crime: Omputer Heft Nauthorised SE Ccess Odification HE Omputer Isuse CTvicrattlehead2013Pas encore d'évaluation
- Nurse Practitioner Board ReviewD'EverandNurse Practitioner Board ReviewÉvaluation : 5 sur 5 étoiles5/5 (1)
- Practice Exam 3Document93 pagesPractice Exam 3Arash SamieiPas encore d'évaluation
- PracticeExam 3 AnsDocument52 pagesPracticeExam 3 AnsBehrouz YariPas encore d'évaluation
- Thyrotoxicosis Ischaemic Heart Disease Hypertension Alcohol Excess Lone Atrial FibrillationDocument5 pagesThyrotoxicosis Ischaemic Heart Disease Hypertension Alcohol Excess Lone Atrial FibrillationZhao Xuan TanPas encore d'évaluation
- 0@media External File 3723Document1 page0@media External File 3723sameePas encore d'évaluation
- 0@media External File 3723 PDFDocument6 pages0@media External File 3723 PDFsamee100% (1)
- AAEM RSA50DrugFactsEveryEPShouldKnow PDFDocument52 pagesAAEM RSA50DrugFactsEveryEPShouldKnow PDFalaam mahmoudPas encore d'évaluation
- Com - Whatsapp.provider - Media Item 18324Document8 pagesCom - Whatsapp.provider - Media Item 18324samee54% (13)
- Downloads All Downloads 1211 PDFDocument6 pagesDownloads All Downloads 1211 PDFsameePas encore d'évaluation
- Org - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFDocument2 pagesOrg - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFsameePas encore d'évaluation
- Org - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5920093559716840840 PDFDocument32 pagesOrg - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5920093559716840840 PDFsameePas encore d'évaluation
- Advance DirectiveDocument14 pagesAdvance DirectivesameePas encore d'évaluation
- Org - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFDocument2 pagesOrg - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFsameePas encore d'évaluation
- Sliding Around: ResultsDocument9 pagesSliding Around: ResultssameePas encore d'évaluation
- 12 CR Use of Tenecteplase ForDocument6 pages12 CR Use of Tenecteplase ForsameePas encore d'évaluation
- Rcem Learning FRCEM PRIMARY Paper 1Document9 pagesRcem Learning FRCEM PRIMARY Paper 1sameePas encore d'évaluation
- 12 CR Use of Tenecteplase For PDFDocument4 pages12 CR Use of Tenecteplase For PDFsameePas encore d'évaluation
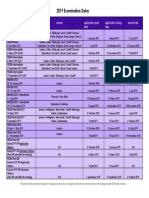
- 2019 Dates For Website - Final 20181220Document1 page2019 Dates For Website - Final 20181220sameePas encore d'évaluation
- THe New Berlin Definition Pneumon, Dec 2012Document4 pagesTHe New Berlin Definition Pneumon, Dec 2012Orion JohnPas encore d'évaluation
- Rapid Sequence InductionDocument8 pagesRapid Sequence InductionAngela Mitchelle NyanganPas encore d'évaluation
- Magnesium SulfateDocument2 pagesMagnesium SulfatesameePas encore d'évaluation
- Rcem Learning FRCEM PRIMARY Paper 3 PDFDocument8 pagesRcem Learning FRCEM PRIMARY Paper 3 PDFsamee0% (1)
- Magnesium SulfateDocument2 pagesMagnesium SulfatesameePas encore d'évaluation
- Never Events List 2018: January 2018Document23 pagesNever Events List 2018: January 2018Elisa NeacsuPas encore d'évaluation
- VNS Faculty of Pharmacy: Mentors - Presented byDocument1 pageVNS Faculty of Pharmacy: Mentors - Presented bypoplu100% (1)
- AFJMediareleasefinal 2Document2 pagesAFJMediareleasefinal 2Sam TormeyPas encore d'évaluation
- Canal-Sealing-Yang-Berbeda: Daftar PustakaDocument4 pagesCanal-Sealing-Yang-Berbeda: Daftar PustakaMichelle LohoPas encore d'évaluation
- SDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionDocument5 pagesSDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionYwagar YwagarPas encore d'évaluation
- MedicalCertificate ExmpleDocument1 pageMedicalCertificate ExmpleJareena SamsonPas encore d'évaluation
- Infiltration, A New Therapy For Masking Enamel White Spot PDFDocument12 pagesInfiltration, A New Therapy For Masking Enamel White Spot PDFwijayanti siswantoPas encore d'évaluation
- Testicular Self ExaminationDocument3 pagesTesticular Self ExaminationMatías DengPas encore d'évaluation
- 1090 - Biology - News Article 2 - Lianna TrevinoDocument2 pages1090 - Biology - News Article 2 - Lianna Trevinoapi-302666758Pas encore d'évaluation
- Fda AmoxicillinDocument18 pagesFda AmoxicillingitapusPas encore d'évaluation
- Farmacist Desk Reference ReviewDocument1 pageFarmacist Desk Reference ReviewThinh DoPas encore d'évaluation
- PMID 1393911 Niacin Vs NiacinamideDocument1 pagePMID 1393911 Niacin Vs NiacinamideInbal LandsbergPas encore d'évaluation
- DM Brochure For NCM 106Document12 pagesDM Brochure For NCM 106Kimsha ConcepcionPas encore d'évaluation
- NSTP Act2 Suan, Allyna ChantalDocument8 pagesNSTP Act2 Suan, Allyna ChantalChan TalPas encore d'évaluation
- Penjagaan Pensiun Dan RealisasinyaDocument11 pagesPenjagaan Pensiun Dan RealisasinyasidoharjoPas encore d'évaluation
- Catheterisation - Suprapubic Catheter ProcedureNewDocument12 pagesCatheterisation - Suprapubic Catheter ProcedureNewAmit KapuriaPas encore d'évaluation
- Intersono IVF ClinicDocument21 pagesIntersono IVF ClinicINTERSONOPas encore d'évaluation
- Various Face Bow Transfer TechniquesDocument49 pagesVarious Face Bow Transfer TechniquesDr.Sathyabhama A.V100% (1)
- ErythromycinDocument1 pageErythromycinKenneth Robert Abrantes0% (1)
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocument7 pagesHANDOUT Chapter 11 Promoting Fetal and Maternal HealthEula ReyesPas encore d'évaluation
- DKA EthiopiaDocument7 pagesDKA EthiopiaBrotherhood of KryptonianPas encore d'évaluation
- The Haunted Self Structural Dissociation and The T PDFDocument7 pagesThe Haunted Self Structural Dissociation and The T PDFKomáromi PéterPas encore d'évaluation
- (IJIT-V7I2P6) :B.Rajalakshmi, G.Sanjana DeviDocument5 pages(IJIT-V7I2P6) :B.Rajalakshmi, G.Sanjana DeviIJITJournalsPas encore d'évaluation
- Mass General Cover LetterDocument1 pageMass General Cover Letterapi-404285262Pas encore d'évaluation
- 1.17 (Surgery) Orthopedic History - Physical ExaminationDocument5 pages1.17 (Surgery) Orthopedic History - Physical ExaminationLeo Mari Go LimPas encore d'évaluation
- Amenorrhoea RemediesDocument8 pagesAmenorrhoea RemediesHomeopathy TorrentsPas encore d'évaluation
- Records and ReportDocument4 pagesRecords and ReportAnusikta PandaPas encore d'évaluation
- Gap Report Astha HospitalDocument49 pagesGap Report Astha HospitalNidhi VijanPas encore d'évaluation
- Progress in Management of The Obstructed AirwayDocument8 pagesProgress in Management of The Obstructed AirwayAnonymous h0DxuJTPas encore d'évaluation
- Quarantine and Isolation Guidance - 1.14.22Document6 pagesQuarantine and Isolation Guidance - 1.14.22Umair Ahmed AbbasiPas encore d'évaluation
- 8 Gene Therapy Alison M BeaneyDocument26 pages8 Gene Therapy Alison M BeaneyDharma DevPas encore d'évaluation