Vous aimerez peut-être aussi
- How To Play The Digital Connect GamesDocument1 pageHow To Play The Digital Connect GamesNarcisa UrsuPas encore d'évaluation
- Abc Data Sheet: Approx. - MinDocument2 pagesAbc Data Sheet: Approx. - MinNarcisa UrsuPas encore d'évaluation
- 10 23 19 Building Bridges SEL - Competencies - 508Document2 pages10 23 19 Building Bridges SEL - Competencies - 508Narcisa UrsuPas encore d'évaluation
- Task Analysis SupplementDocument26 pagesTask Analysis SupplementNarcisa Ursu100% (1)
- Task Analysis SupplementDocument26 pagesTask Analysis SupplementNarcisa Ursu100% (1)
- Reglarea Emotionala - MonografieDocument148 pagesReglarea Emotionala - Monografielola100% (1)
- Why A Person With An IQ of 140 Works For A Person With An IQ of 90?Document2 pagesWhy A Person With An IQ of 140 Works For A Person With An IQ of 90?Narcisa UrsuPas encore d'évaluation
- Tour TheDocument2 pagesTour TheNarcisa UrsuPas encore d'évaluation
- Positive Discipline ManualDocument356 pagesPositive Discipline ManualNarcisa Ursu100% (3)
- Guidance DisciplineDocument43 pagesGuidance DisciplineNarcisa UrsuPas encore d'évaluation
- Discipline and The Child With Tourette's SyndromeDocument9 pagesDiscipline and The Child With Tourette's SyndromeNarcisa UrsuPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Fgei AdDocument4 pagesFgei Adyisidep991Pas encore d'évaluation
- Account Statement 05 01 2021 PDFDocument1 pageAccount Statement 05 01 2021 PDFGabiMalaquiasPas encore d'évaluation
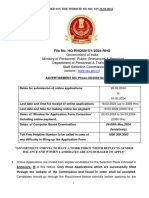
- Phase-XII Notification 2024 26022024Document167 pagesPhase-XII Notification 2024 26022024s71397586Pas encore d'évaluation
- Judie A. Compas: With HonorsDocument10 pagesJudie A. Compas: With HonorsGRACE VERIDIANOPas encore d'évaluation
- Explicit InstructionDocument16 pagesExplicit InstructionNette Cervantes100% (1)
- FORM-1 RayanaDocument2 pagesFORM-1 RayanaIan ElviniaPas encore d'évaluation
- Analisis Kemampuan Pemecahan Masalah Matematis Materi PolinomialDocument10 pagesAnalisis Kemampuan Pemecahan Masalah Matematis Materi PolinomialLAILY YASMIN QODRIYAH 2019Pas encore d'évaluation
- TLE 10 - DLL Q4 Week 5 - HAIR DRESSINGDocument4 pagesTLE 10 - DLL Q4 Week 5 - HAIR DRESSINGjomarie estibalPas encore d'évaluation
- GCAS 09 Rizal Semi-Final ActivityDocument2 pagesGCAS 09 Rizal Semi-Final Activityeureka faderogaoPas encore d'évaluation
- NEET UG 2022 Merit List Round 1Document39 pagesNEET UG 2022 Merit List Round 1Utsab DasPas encore d'évaluation
- ProQuestDocuments 2021-11-24Document6 pagesProQuestDocuments 2021-11-24Accurate Technology LimitedPas encore d'évaluation
- My Space Creating Enabling Environments For Young ChildrenDocument36 pagesMy Space Creating Enabling Environments For Young ChildrenLuciennePas encore d'évaluation
- Alfonso, Michael John Agaser 202005047MN0 Bachelor of Science in Electrical Engineering Enrolled SubjectsDocument1 pageAlfonso, Michael John Agaser 202005047MN0 Bachelor of Science in Electrical Engineering Enrolled SubjectsMJA.AlfonsoPas encore d'évaluation
- The National Education PolicyDocument3 pagesThe National Education Policysofia guptaPas encore d'évaluation
- Lesson Plan 6GDocument4 pagesLesson Plan 6GNguyen LinhPas encore d'évaluation
- Chapter 3 Biomechanics KINE 3300Document110 pagesChapter 3 Biomechanics KINE 3300Selviya AvaurumPas encore d'évaluation
- Educational System of The Selected CountriesDocument34 pagesEducational System of The Selected CountriesAndre Ron Jerome UndalokPas encore d'évaluation
- English Year3 Grammar Articles Lesson PlanDocument6 pagesEnglish Year3 Grammar Articles Lesson PlanIlham Izzat100% (3)
- Considerando El Futuro de La ProfesionDocument52 pagesConsiderando El Futuro de La ProfesionTania BeltranPas encore d'évaluation
- Nursery High School: Division of City SchoolsDocument3 pagesNursery High School: Division of City SchoolsEMILIO CARPIOPas encore d'évaluation
- Bosman Et Al-2016-British Journal of Educational TechnologyDocument10 pagesBosman Et Al-2016-British Journal of Educational TechnologyLucía CironaPas encore d'évaluation
- Pragati Degree 2020-21Document179 pagesPragati Degree 2020-21Hgkdb S9plusPas encore d'évaluation
- I Can Smell, Taste and Touch.: Kindergarte N Lesson PlanDocument10 pagesI Can Smell, Taste and Touch.: Kindergarte N Lesson PlanJulhan GubatPas encore d'évaluation
- Why Do Teachers Assign Homework On The WeekendsDocument6 pagesWhy Do Teachers Assign Homework On The Weekendscfhwk3nc100% (1)
- Brigada Eskwela Proposal 2022Document3 pagesBrigada Eskwela Proposal 2022KATHLEEN JOY PABALAY100% (1)
- ResumEsq. Proyecto Max PlanckDocument20 pagesResumEsq. Proyecto Max PlanckLeonardo ArayaPas encore d'évaluation
- Learning Action Cell (Lac) Session Plan School Year 2021 - 2022Document3 pagesLearning Action Cell (Lac) Session Plan School Year 2021 - 2022Nymfreda Lequip100% (1)
- English 7 Q2 Module 1Document17 pagesEnglish 7 Q2 Module 1marjunampoPas encore d'évaluation
- MuseumDocument14 pagesMuseumieltswritingmodulePas encore d'évaluation
- Resolution of ThanksDocument3 pagesResolution of ThanksJoarichPas encore d'évaluation