Vous aimerez peut-être aussi
- Clinical Case Scenario 6Document17 pagesClinical Case Scenario 6Sean Menard Flores100% (1)
- KetoprofenDocument22 pagesKetoprofenRickPas encore d'évaluation
- Careplan Medication ListDocument17 pagesCareplan Medication ListGiorgia ScorsonePas encore d'évaluation
- 2023 Free 120Document65 pages2023 Free 120Edmund BlackadderPas encore d'évaluation
- 10-TCT 2012fyughklDocument196 pages10-TCT 2012fyughklMuhammed BarznjiPas encore d'évaluation
- Enteral Nutrition (Gastrojejunotomy)Document30 pagesEnteral Nutrition (Gastrojejunotomy)Hairul IzlanPas encore d'évaluation
- MucosolvanDocument2 pagesMucosolvanAyah Paasa100% (1)
- Silymarin PharmacologyDocument18 pagesSilymarin PharmacologySilky Pradeep KumarPas encore d'évaluation
- Tishk International University: ApixabanDocument4 pagesTishk International University: ApixabanDyar MzafarPas encore d'évaluation
- Commentary Biowaiver Monographs For Immediate Release Solid Oral Dosage Forms: PrednisoloneDocument20 pagesCommentary Biowaiver Monographs For Immediate Release Solid Oral Dosage Forms: PrednisolonePrisca WicitaPas encore d'évaluation
- Drugs For EmergencyDocument25 pagesDrugs For EmergencyJunathan L. DelgadoPas encore d'évaluation
- Mesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidDocument4 pagesMesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidAnkan PalPas encore d'évaluation
- Arabic Exam 4 - 1Document6 pagesArabic Exam 4 - 1Lowry GuettaPas encore d'évaluation
- Common Drugs Use in OphthalmologyDocument40 pagesCommon Drugs Use in Ophthalmologyณัช เกษมPas encore d'évaluation
- Pharmacology of DiureticsDocument75 pagesPharmacology of DiureticsAhmed BassettPas encore d'évaluation
- Clinical Pharmacy Lab - Quiz Part 2Document4 pagesClinical Pharmacy Lab - Quiz Part 2Aassh DcmbrPas encore d'évaluation
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- 874 Hepa Merz 1331899928 PDFDocument1 page874 Hepa Merz 1331899928 PDFSanjay NavalePas encore d'évaluation
- Nifedipine Uses, Dosage & Side EffectsDocument6 pagesNifedipine Uses, Dosage & Side EffectsXICMENPas encore d'évaluation
- AugmentinDocument24 pagesAugmentinKaren Ann M. EstradaPas encore d'évaluation
- 1.1 Extemporaneous Compounded Drugs - HPREDocument5 pages1.1 Extemporaneous Compounded Drugs - HPREKianna Marie MuyotPas encore d'évaluation
- Anticholinergics Study Drug ListDocument1 pageAnticholinergics Study Drug ListDrima Edi100% (1)
- Innovation in Capsule Dosage FormDocument69 pagesInnovation in Capsule Dosage FormAshish Gajera100% (1)
- Types of Parenteral ProductsDocument7 pagesTypes of Parenteral ProductsJoginder KumarPas encore d'évaluation
- BrivaracetamDocument110 pagesBrivaracetamBendisDacicaPas encore d'évaluation
- LiverTox: Clinical and Research Information On Drug-Induced Liver Injury - AcetaminophenDocument41 pagesLiverTox: Clinical and Research Information On Drug-Induced Liver Injury - AcetaminophenJessica AristaPas encore d'évaluation
- EMERGENCY DRUGS: A Drug StudyDocument8 pagesEMERGENCY DRUGS: A Drug StudyShaine WolfePas encore d'évaluation
- Mini RinDocument5 pagesMini Rinlovely_dyaPas encore d'évaluation
- InsulinDocument1 pageInsulinamaliea234Pas encore d'évaluation
- Drug OmeprazoleDocument1 pageDrug OmeprazoleSrkocherPas encore d'évaluation
- Daflon Addition in Treatment Coventional MedicalDocument8 pagesDaflon Addition in Treatment Coventional MedicalTha Vila Le ColloPas encore d'évaluation
- Drug PrilosecDocument1 pageDrug PrilosecSrkocher100% (1)
- RoD and BioavailibilityDocument37 pagesRoD and BioavailibilityDzil FikriPas encore d'évaluation
- VasopressinDocument2 pagesVasopressinKim LompotPas encore d'évaluation
- MenopurDocument7 pagesMenopurSimran KaurPas encore d'évaluation
- Magnesium Hydroxide (Milk of Magnesia)Document1 pageMagnesium Hydroxide (Milk of Magnesia)EPas encore d'évaluation
- Zyloprim Drug CardDocument1 pageZyloprim Drug CardSheri490Pas encore d'évaluation
- Pharmacology: Nepthali Christuar Aldueza, R.N. Calamba Doctors CollegeDocument49 pagesPharmacology: Nepthali Christuar Aldueza, R.N. Calamba Doctors CollegeArielle Joy Atienza100% (1)
- Stimulates Peripheral Glucose Uptake, Inhibits Hepatic Glucose Production, Inhibits Lipolysis and Proteolysis, Regulating Glucose MetabolismDocument4 pagesStimulates Peripheral Glucose Uptake, Inhibits Hepatic Glucose Production, Inhibits Lipolysis and Proteolysis, Regulating Glucose MetabolismKey CelestinoPas encore d'évaluation
- Adult Parenteral Guidelines 2020Document57 pagesAdult Parenteral Guidelines 2020Sara Aly YoussefPas encore d'évaluation
- Nonsteroidal Anti-Inflamatory DrugsDocument4 pagesNonsteroidal Anti-Inflamatory DrugsYogi drPas encore d'évaluation
- Drug Study: ER DrugsDocument5 pagesDrug Study: ER Drugsmaeca101Pas encore d'évaluation
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoPas encore d'évaluation
- Daptomycin (Cubicin)Document1 pageDaptomycin (Cubicin)Adrianne BazoPas encore d'évaluation
- Final Answer of PharmacologyDocument45 pagesFinal Answer of Pharmacologynidhhu100% (1)
- AzathioprineDocument3 pagesAzathioprineAdela abboudPas encore d'évaluation
- (Generic Name) ® Drotaverine 40mgDocument2 pages(Generic Name) ® Drotaverine 40mgSangar Sardar100% (1)
- Transdermal Drug Delivery System - ManufDocument13 pagesTransdermal Drug Delivery System - ManufEsther Faith GabrielPas encore d'évaluation
- 2020 Ed Dilution ProtocolDocument72 pages2020 Ed Dilution ProtocolTuan SharatulPas encore d'évaluation
- IsoprenalineDocument2 pagesIsoprenalineImmanuel Victor GeorgePas encore d'évaluation
- ParacetamolDocument78 pagesParacetamolMichalPas encore d'évaluation
- Case Study - Plan B Oral ContraceptiveDocument27 pagesCase Study - Plan B Oral ContraceptiveAiza AyazPas encore d'évaluation
- PharmacokineticsDocument7 pagesPharmacokineticsJan KarnowskiPas encore d'évaluation
- Didanosine PDFDocument6 pagesDidanosine PDFFilda SetyaPas encore d'évaluation
- Pharmacokinetic ParametersDocument37 pagesPharmacokinetic ParametersAyesha InamPas encore d'évaluation
- Drug CardsDocument3 pagesDrug CardsDave HillPas encore d'évaluation
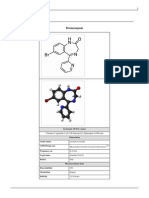
- BromazepamDocument6 pagesBromazepamMariusNeicuPas encore d'évaluation
- Xylocard PiDocument11 pagesXylocard PiRamakant SharmaPas encore d'évaluation
- Availability: Classifications: Central Nervous System Agent Nsaid (Cox-1) Analgesic Antipyretic Pregnancy Category: BDocument4 pagesAvailability: Classifications: Central Nervous System Agent Nsaid (Cox-1) Analgesic Antipyretic Pregnancy Category: BCay SevillaPas encore d'évaluation
- AlbuterolDocument1 pageAlbuterolCassiePas encore d'évaluation
- Drug DilantinDocument1 pageDrug DilantinSrkocherPas encore d'évaluation
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingD'EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováPas encore d'évaluation
- Drug Study AdalatDocument4 pagesDrug Study AdalatLea CelestialPas encore d'évaluation
- Medication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Document43 pagesMedication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Kath Rubio0% (1)
- 100021121Document2 pages100021121Di Icu SekarangPas encore d'évaluation
- Penawaran 2015-2018 1Document46 pagesPenawaran 2015-2018 1Anton RisparyantoPas encore d'évaluation
- Physio Assess Form Oct 2022Document5 pagesPhysio Assess Form Oct 2022RishaadPas encore d'évaluation
- RNCM 101 Guidelines For Return Demonstration 2021Document24 pagesRNCM 101 Guidelines For Return Demonstration 2021Athena AlabadoPas encore d'évaluation
- Ier Pe ADocument27 pagesIer Pe ATrixia Delgado100% (1)
- Cardiac Tamponade 2Document23 pagesCardiac Tamponade 2Jethro Floyd QuintoPas encore d'évaluation
- Harrisons Lecture Notes Part12 Sections2and3Document24 pagesHarrisons Lecture Notes Part12 Sections2and3adevasenPas encore d'évaluation
- 2020 Acc Hocm GuidelinesDocument16 pages2020 Acc Hocm GuidelinesdanniPas encore d'évaluation
- F3 Chapter 3 TransportationDocument19 pagesF3 Chapter 3 TransportationJue Hazea GoldshopPas encore d'évaluation
- Sindroma NefrotikDocument36 pagesSindroma NefrotikjustrudinPas encore d'évaluation
- Normal Chest RadiographDocument108 pagesNormal Chest RadiographVenu Madhav100% (1)
- Circulation BioHackDocument9 pagesCirculation BioHackManav SinghPas encore d'évaluation
- Krok 1 Medicine 2014Document24 pagesKrok 1 Medicine 2014bose_lowe11Pas encore d'évaluation
- ECMO, Adults BJA 2011Document5 pagesECMO, Adults BJA 2011RAGHAVENDRA VAGYANNAVARPas encore d'évaluation
- Level of Organisation QPDocument10 pagesLevel of Organisation QPViviana PlacentinoPas encore d'évaluation
- Creatinine ClearanceDocument6 pagesCreatinine ClearancedianaPas encore d'évaluation
- Cardio VacDocument6 pagesCardio VacstarzecPas encore d'évaluation
- Labortory Test or ManeuverDocument2 pagesLabortory Test or ManeuverJeno Luis J. ACUBPas encore d'évaluation
- Physio CAT 2 AnsweredDocument34 pagesPhysio CAT 2 AnsweredJohn KennedyPas encore d'évaluation
- Compartment SyndromeDocument21 pagesCompartment SyndromeMiztaloges86100% (1)
- Infective EndocarditisDocument18 pagesInfective EndocarditisSam100% (1)
- Aortic StenosisDocument19 pagesAortic StenosisPraveen RamasamyPas encore d'évaluation
- Stress-Induced (Takotsubo) CardiomyopathyDocument13 pagesStress-Induced (Takotsubo) CardiomyopathyAdrian GeambasuPas encore d'évaluation
- Referred PainDocument10 pagesReferred Paindina sharafPas encore d'évaluation
- Multidetector-Row CT Angiography PDFDocument212 pagesMultidetector-Row CT Angiography PDFS KALYAN100% (2)
- Lipid Metabolism: Prof. Talal Abdulrazzaq AlkawryDocument39 pagesLipid Metabolism: Prof. Talal Abdulrazzaq AlkawryRami GhalibPas encore d'évaluation