Vous aimerez peut-être aussi
- Ergonomic Analysis of Construction Jobs in India: A Biomechanical Modelling ApproachDocument7 pagesErgonomic Analysis of Construction Jobs in India: A Biomechanical Modelling ApproachBERLIAN ANNISA NUR RAHMASARIPas encore d'évaluation
- Wearable Insole Presure System For Automated Detection and Clasification of Awkward Working Postures in Construction WorkersDocument10 pagesWearable Insole Presure System For Automated Detection and Clasification of Awkward Working Postures in Construction WorkersErik Satrya WijayaPas encore d'évaluation
- 1 s2.0 S0926580518304138 MainDocument15 pages1 s2.0 S0926580518304138 MainYona NurhalizaPas encore d'évaluation
- Sustainability 14 04356 v2Document19 pagesSustainability 14 04356 v2maisurah iskandar maiPas encore d'évaluation
- Biomechanical Investigation of Human Femur by Reverse Engineering As A Robust Method and Applied SimplificationsDocument7 pagesBiomechanical Investigation of Human Femur by Reverse Engineering As A Robust Method and Applied Simplificationsimen mehriPas encore d'évaluation
- A Twenty-Year Retrospective Analysis of Risk Assessment of Biomechanical Overload of The Upper Limbs in Multiple Occupational Settings Comparison of Different Ergonomic MethodsDocument13 pagesA Twenty-Year Retrospective Analysis of Risk Assessment of Biomechanical Overload of The Upper Limbs in Multiple Occupational Settings Comparison of Different Ergonomic MethodsRai ParedesPas encore d'évaluation
- Status Survey of Occupational Risk Factors of Manual Material Handling Tasks at A Construction Site in IndiaDocument8 pagesStatus Survey of Occupational Risk Factors of Manual Material Handling Tasks at A Construction Site in IndiaTirta AjiPas encore d'évaluation
- References ErgoDocument13 pagesReferences ErgomizanPas encore d'évaluation
- Biomechanical Modelling of Manual Material Handling Tasks: A Comprehensive ReviewDocument8 pagesBiomechanical Modelling of Manual Material Handling Tasks: A Comprehensive ReviewTirta AjiPas encore d'évaluation
- Machine Learning in Manufacturing Ergonomics Recent Advances Challenges and OpportunitiesDocument8 pagesMachine Learning in Manufacturing Ergonomics Recent Advances Challenges and OpportunitiesFARHANAH ALMIRAH NADILA -Pas encore d'évaluation
- Int J Industrial Ergonomics Version FinaleDocument16 pagesInt J Industrial Ergonomics Version FinaleThảo DươngPas encore d'évaluation
- WishaDocument12 pagesWishaRisnaldi Nur HakikiPas encore d'évaluation
- The Incorporation of Virtual Ergonomics To ImproveDocument9 pagesThe Incorporation of Virtual Ergonomics To ImproveMuthu BaskaranPas encore d'évaluation
- Uncorrected Author ProofDocument16 pagesUncorrected Author ProofHeaven in Home StudentPas encore d'évaluation
- 2019, Evaluation of Ergonomic Working Conditions Among Standing Sewing Workstation in Sri LankaDocument14 pages2019, Evaluation of Ergonomic Working Conditions Among Standing Sewing Workstation in Sri LankaEyob MinbalePas encore d'évaluation
- Synopsis KwdsboqDocument9 pagesSynopsis Kwdsboqdivya.bishnoi8Pas encore d'évaluation
- Enhancing Workplace Safetywith Ergonomic Assessments Using REBAand RULAPoweredby Computer Vision TechnologyDocument8 pagesEnhancing Workplace Safetywith Ergonomic Assessments Using REBAand RULAPoweredby Computer Vision TechnologyberliancantikberlianPas encore d'évaluation
- Fall Prevention From Ladders Utilizing ADocument18 pagesFall Prevention From Ladders Utilizing Ayazhini shanmugamPas encore d'évaluation
- Implementation of Rapid Upper Limb Assessment Technique in Automotive Parts Manufacturing IndustryDocument4 pagesImplementation of Rapid Upper Limb Assessment Technique in Automotive Parts Manufacturing IndustryEduardo CapeletiPas encore d'évaluation
- A Review of The NIOSH Lifting Equation and ErgonomDocument8 pagesA Review of The NIOSH Lifting Equation and ErgonomJoana AraújoPas encore d'évaluation
- An Approach To Analyze Human Caused Work ErrorsDocument6 pagesAn Approach To Analyze Human Caused Work Errorsencuesta.doctorado2023Pas encore d'évaluation
- An Ergonomic Study For 6S Workplace ImprovementDocument6 pagesAn Ergonomic Study For 6S Workplace ImprovementAnonymous 5YMOxVQPas encore d'évaluation
- Paper FD With RL 2Document30 pagesPaper FD With RL 2Majd SaiedPas encore d'évaluation
- Ergonomic Risk Assessment of Workers in Garment IndustryDocument7 pagesErgonomic Risk Assessment of Workers in Garment IndustryEngrWasiAhmadPas encore d'évaluation
- Manual Material Handling Assessment and Repetitive Tasks With Two Methods MAC and ART in A Subsidiary of A Manufacturer of Cleaning Products A R T I C L E InfoDocument9 pagesManual Material Handling Assessment and Repetitive Tasks With Two Methods MAC and ART in A Subsidiary of A Manufacturer of Cleaning Products A R T I C L E InfoNORERNY SHUHADA BINTI HAMDANPas encore d'évaluation
- Dynamic Biomechanical Analysis For Construction Tasks Using Motion Data From Vision-Based Motion Capture ApproachesDocument8 pagesDynamic Biomechanical Analysis For Construction Tasks Using Motion Data From Vision-Based Motion Capture ApproachesMiko Ta KomePas encore d'évaluation
- Journal AssignmentNewDocument14 pagesJournal AssignmentNewSAWIK MEHMOODPas encore d'évaluation
- Ergonomic Evaluation and Axiomatic Design of Manual Material Handling Activity For Medium Scale IndustryDocument10 pagesErgonomic Evaluation and Axiomatic Design of Manual Material Handling Activity For Medium Scale IndustryAmit BankarPas encore d'évaluation
- Evaluation - of - Safety - and - Health - Performance - On - Con KulaDocument11 pagesEvaluation - of - Safety - and - Health - Performance - On - Con KulaabdirahmanPas encore d'évaluation
- Mohammed2020 Article ErgonomicAnalysisOfAWorkingPosDocument8 pagesMohammed2020 Article ErgonomicAnalysisOfAWorkingPostemesgen DemssiePas encore d'évaluation
- 1 s2.0 S0167473020301107 MainDocument14 pages1 s2.0 S0167473020301107 MainArif SantosoPas encore d'évaluation
- Ergonomic Evaluation of The Work Stations in A Garment Manufacturing Industry-An Exploratory StudyDocument5 pagesErgonomic Evaluation of The Work Stations in A Garment Manufacturing Industry-An Exploratory StudyAnshu RoyPas encore d'évaluation
- Construction Job Safety AnalysisDocument8 pagesConstruction Job Safety AnalysisMohd Yazid Mohamad Yunus100% (1)
- Analysis The Awkward Posture Ergonomic Risk and WoDocument7 pagesAnalysis The Awkward Posture Ergonomic Risk and WoCHOIRPas encore d'évaluation
- Design and Evaluation of Ergonomic Interventions For The Prevention of Musculoskeletal Disorders in IndiaDocument7 pagesDesign and Evaluation of Ergonomic Interventions For The Prevention of Musculoskeletal Disorders in IndiaRenaldiPrimaSaputraPas encore d'évaluation
- 0c96051c575a75b5e4000000 PDFDocument8 pages0c96051c575a75b5e4000000 PDFMatheus SouzaPas encore d'évaluation
- Work Posture Risk Comparison of RULA and REBA BaseDocument10 pagesWork Posture Risk Comparison of RULA and REBA BaseberliancantikberlianPas encore d'évaluation
- Lifting Equation For Manual LiftingDocument10 pagesLifting Equation For Manual LiftingShafiqul IslamPas encore d'évaluation
- 2019 - Joshi - A Systematic Review of Comparative Studies On Ergonomic Assessment TechniquesDocument14 pages2019 - Joshi - A Systematic Review of Comparative Studies On Ergonomic Assessment TechniquesJohannes SchützPas encore d'évaluation
- Risk AssesmentDocument13 pagesRisk AssesmentORIENT YOUR CAREERPas encore d'évaluation
- Application of Lean Six Sigma Tools To Minimize Length of Stay For Ophthalmology Day Case Surgery PDFDocument18 pagesApplication of Lean Six Sigma Tools To Minimize Length of Stay For Ophthalmology Day Case Surgery PDFM HPas encore d'évaluation
- 50-Article Text-145-107-10-20210622Document30 pages50-Article Text-145-107-10-20210622Hazeq ZPas encore d'évaluation
- A Framework For Crane Selection in Large-Scale Industrial Construction ProjectsDocument9 pagesA Framework For Crane Selection in Large-Scale Industrial Construction ProjectsAnggy de RinconPas encore d'évaluation
- Ergonomic Evaluation To Improve Work Posture IJERTV5IS031136Document9 pagesErgonomic Evaluation To Improve Work Posture IJERTV5IS031136NIRAJ NARSINGDAS BHATTADPas encore d'évaluation
- Validation of The Lifft Risk Assessment Tool and Guidance On Its UseDocument10 pagesValidation of The Lifft Risk Assessment Tool and Guidance On Its UsehigormePas encore d'évaluation
- Materials Today: Proceedings: Harold Villacís Jara, Iván Zambrano Orejuela, J.M. Baydal-BertomeuDocument7 pagesMaterials Today: Proceedings: Harold Villacís Jara, Iván Zambrano Orejuela, J.M. Baydal-Bertomeumari ccallo noaPas encore d'évaluation
- Comparison Reba and QecDocument7 pagesComparison Reba and Qecm_myfrenPas encore d'évaluation
- Assessing - Risk - in - Sustainable - Constructi20161122 3176 f946pb With Cover Page v2Document16 pagesAssessing - Risk - in - Sustainable - Constructi20161122 3176 f946pb With Cover Page v2Fatih GülenPas encore d'évaluation
- Assessment of Ergonomics Risk Experienced by Welding Workers in A Rail Component Manufacturing OrganizationDocument10 pagesAssessment of Ergonomics Risk Experienced by Welding Workers in A Rail Component Manufacturing OrganizationcanavaroyunculukPas encore d'évaluation
- QEC (Quick Exposure Check) : General Description and Development of The MethodDocument4 pagesQEC (Quick Exposure Check) : General Description and Development of The MethodmulyadiPas encore d'évaluation
- Introducing Quantitative Analysis Methods Into Virtual Environments For Real-Time and Continuous Ergonomic EvaluationsDocument14 pagesIntroducing Quantitative Analysis Methods Into Virtual Environments For Real-Time and Continuous Ergonomic EvaluationsJorge Luis Raygada AzpilcuetaPas encore d'évaluation
- A Review On Ergonomic Risk Factors Causing Musculoskeletal Disorders Among Construction Workers IJERTV9IS060887Document3 pagesA Review On Ergonomic Risk Factors Causing Musculoskeletal Disorders Among Construction Workers IJERTV9IS060887Jeisther Timothy GalanoPas encore d'évaluation
- Personnel Functional Safety CertificationDocument15 pagesPersonnel Functional Safety CertificationjeebsPas encore d'évaluation
- Postural Analysis of Building Construction Workers Using ErgonomicsDocument9 pagesPostural Analysis of Building Construction Workers Using Ergonomicsgowri ajithPas encore d'évaluation
- 2018-Proactive Fall Safety ManagementDocument11 pages2018-Proactive Fall Safety ManagementMohd ShafiqPas encore d'évaluation
- 2012 Elsevier MaterialsScienceandEngineeringA Aminallahp3 Vol.538pages2027Document9 pages2012 Elsevier MaterialsScienceandEngineeringA Aminallahp3 Vol.538pages2027Israel AliagaPas encore d'évaluation
- Ibrahim 2020 IOP Conf. Ser. Mater. Sci. Eng. 834 012056 PDFDocument7 pagesIbrahim 2020 IOP Conf. Ser. Mater. Sci. Eng. 834 012056 PDFerlangga naurianPas encore d'évaluation
- 2019 - Cerqueira - Instrument Based Ergonomic Assessment A Perspective On The Current State of Art and Future TrendsDocument4 pages2019 - Cerqueira - Instrument Based Ergonomic Assessment A Perspective On The Current State of Art and Future TrendsJohannes SchützPas encore d'évaluation
- Residual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentD'EverandResidual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentPas encore d'évaluation
- Textile Wastewater Treatment:, IncludingDocument8 pagesTextile Wastewater Treatment:, IncludingSze ZhaoPas encore d'évaluation
- Methodology For Performance Analysis of Textile Ef Uent Treatment Plants in BangladeshDocument7 pagesMethodology For Performance Analysis of Textile Ef Uent Treatment Plants in BangladeshSze ZhaoPas encore d'évaluation
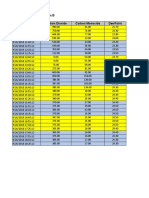
- Logged Data Chart Location B Carbon Dioxide Carbon Monoxide Dewpoint TimestampDocument4 pagesLogged Data Chart Location B Carbon Dioxide Carbon Monoxide Dewpoint TimestampSze ZhaoPas encore d'évaluation
- PM2 5Document2 pagesPM2 5Sze ZhaoPas encore d'évaluation
- Location B TVOC Against TimeDocument2 pagesLocation B TVOC Against TimeSze ZhaoPas encore d'évaluation
- Environmental Management Systems (EMS) Adoption in Sarawak (Malaysia) : Implementation MotivationsDocument19 pagesEnvironmental Management Systems (EMS) Adoption in Sarawak (Malaysia) : Implementation MotivationsSze ZhaoPas encore d'évaluation
- IAL Mathematics Formula BookDocument34 pagesIAL Mathematics Formula BookHaleef Mk0% (1)
- Mechanical Engineering Department University of Engineering and Technology, LahoreDocument22 pagesMechanical Engineering Department University of Engineering and Technology, LahoreSyed MunawarPas encore d'évaluation
- Navigating The Complexities of Modern SocietyDocument2 pagesNavigating The Complexities of Modern SocietytimikoPas encore d'évaluation
- Case Study of Master of Business AdminisDocument8 pagesCase Study of Master of Business AdminisYoke MalondaPas encore d'évaluation
- Histology SlidesDocument47 pagesHistology SlidesHaJoRaPas encore d'évaluation
- 02 - Financial Accounting - Accounts Receivable ReportsDocument28 pages02 - Financial Accounting - Accounts Receivable ReportsjohnPas encore d'évaluation
- Test Bank For Economic Development The Pearson Series in Economics 11th Edition Michael P TodaroDocument24 pagesTest Bank For Economic Development The Pearson Series in Economics 11th Edition Michael P TodaroRebeccaRodriguezcqgf100% (49)
- Literacy Planning Sheet Year Group: Reception Stimulus: Jolly Phonics Day Skill Learning Objective Main Teaching Focused Task(s) Key Skill 1Document2 pagesLiteracy Planning Sheet Year Group: Reception Stimulus: Jolly Phonics Day Skill Learning Objective Main Teaching Focused Task(s) Key Skill 1Engy HassanPas encore d'évaluation
- REELY Chapter 7 Flashcards - QuizletDocument2 pagesREELY Chapter 7 Flashcards - QuizletCERTIFIED TROLLPas encore d'évaluation
- Ifc 8thconf 4c4papDocument29 pagesIfc 8thconf 4c4papgauravpassionPas encore d'évaluation
- The Importance of Will and Moral CourageDocument4 pagesThe Importance of Will and Moral CourageCharles Justin C. SaldiPas encore d'évaluation
- Designing User-Centered Decision Support Tools For AgricultureDocument17 pagesDesigning User-Centered Decision Support Tools For AgricultureCABIPas encore d'évaluation
- Veta 5 - Datasheet - ENG - 20210315Document3 pagesVeta 5 - Datasheet - ENG - 20210315JuanPas encore d'évaluation
- Uw Math Stat394 Hw4 SolDocument4 pagesUw Math Stat394 Hw4 SolRizsPas encore d'évaluation
- SAQOL 39 Proxy Version Sr55z7Document5 pagesSAQOL 39 Proxy Version Sr55z7Fernanda VegaPas encore d'évaluation
- Role of Geotechnical Properties of Soil On Civil Engineering StructuresDocument8 pagesRole of Geotechnical Properties of Soil On Civil Engineering StructuresSaša MarinPas encore d'évaluation
- Topic 1Document11 pagesTopic 1Mercy MissionPas encore d'évaluation
- Music Laptop Script (WhiteHat JR Customers)Document3 pagesMusic Laptop Script (WhiteHat JR Customers)Yash JainPas encore d'évaluation
- The Mystery of Berry Berenson and 9-11Document5 pagesThe Mystery of Berry Berenson and 9-11HierocrypticPas encore d'évaluation
- My Strengths WorksheetDocument5 pagesMy Strengths WorksheetvilavanadonisPas encore d'évaluation
- Cable For Solar Power SystemDocument1 pageCable For Solar Power SystemEnspartan 63Pas encore d'évaluation
- Engineering Standards FOR Units Original Edition AUG. 1993: IPS-E-GN-100Document81 pagesEngineering Standards FOR Units Original Edition AUG. 1993: IPS-E-GN-100Pouya ZakerabbasiPas encore d'évaluation
- Rock Reinforcement Modelling - Cable Bolts in PLAXIS 2DDocument12 pagesRock Reinforcement Modelling - Cable Bolts in PLAXIS 2Dchaymaa MRHARPas encore d'évaluation
- MEE20004 Structural Mechanics Outline Sem 2 2023Document11 pagesMEE20004 Structural Mechanics Outline Sem 2 2023MKPas encore d'évaluation
- Non Heat Treatable Commercial-Purity Aluminium 1050 A: Chemical Composition Limits (In %) Aluminium 99,5% MinimumDocument1 pageNon Heat Treatable Commercial-Purity Aluminium 1050 A: Chemical Composition Limits (In %) Aluminium 99,5% Minimumprivate 2Pas encore d'évaluation
- Tantasqua Regional High School Staff Directory: AdministrationDocument4 pagesTantasqua Regional High School Staff Directory: AdministrationLauren RockPas encore d'évaluation
- Ravi Shankar's Birth Chart / Kundali: Astrological Services For Accurate Answers and Better FeatureDocument1 pageRavi Shankar's Birth Chart / Kundali: Astrological Services For Accurate Answers and Better FeatureEd ReesPas encore d'évaluation
- Instructions:: Exam Papers Must Not Be Removed From The Exam Room Examiners: R.Russo T.KreouzisDocument9 pagesInstructions:: Exam Papers Must Not Be Removed From The Exam Room Examiners: R.Russo T.KreouziszcaptPas encore d'évaluation
- How Fast and Which Way?: Friday 13 October MR PatelDocument20 pagesHow Fast and Which Way?: Friday 13 October MR PatelBenjamin WatsonPas encore d'évaluation
- 2020 Oulade The Neural Basis of Language DevelopmentDocument7 pages2020 Oulade The Neural Basis of Language DevelopmentzonilocaPas encore d'évaluation