Vous aimerez peut-être aussi
- Diseases of Skeletal Muscle FinalDocument30 pagesDiseases of Skeletal Muscle FinalclaudiaPas encore d'évaluation
- JNC 7 PDFDocument104 pagesJNC 7 PDFbellaPas encore d'évaluation
- Slide ModeloDocument48 pagesSlide ModeloIago Moura100% (1)
- WHO Doc On Pediatric IllnessesDocument399 pagesWHO Doc On Pediatric IllnessesUlanda SinghPas encore d'évaluation
- Clinical Lab Reference RangesDocument2 pagesClinical Lab Reference RangessarwarrosunPas encore d'évaluation
- Pediatrics: A Resource GuideDocument35 pagesPediatrics: A Resource GuideKarl Martin PinedaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Introduction To Analog and Digital CommunicationsDocument80 pagesIntroduction To Analog and Digital CommunicationsvijaPas encore d'évaluation
- Centrifugal Pump Hand BookDocument150 pagesCentrifugal Pump Hand Bookbarun1977100% (2)
- Audit and EnforcementDocument684 pagesAudit and EnforcementmoparthiPas encore d'évaluation
- Practice Test 13Document3 pagesPractice Test 13anhkiett27112008Pas encore d'évaluation
- Waste MGMT Research PPRDocument6 pagesWaste MGMT Research PPRRohit Amorso RanjanPas encore d'évaluation
- PEFA Regional Government of SomaliDocument172 pagesPEFA Regional Government of SomaliGirmaye HailePas encore d'évaluation
- Openlectures Publicity PackDocument20 pagesOpenlectures Publicity PacksuhangdageekPas encore d'évaluation
- Winpepi Sample SizeDocument2 pagesWinpepi Sample SizeHammad RasheedPas encore d'évaluation
- Gildan - Asia - 2019 Catalogue - English - LR PDFDocument21 pagesGildan - Asia - 2019 Catalogue - English - LR PDFKoet Ji CesPas encore d'évaluation
- MF AXIOM Cyber Brief PDFDocument2 pagesMF AXIOM Cyber Brief PDFluis demetrio martinez ruizPas encore d'évaluation
- IGCSE Syllabus Checklist - ICT (0417)Document15 pagesIGCSE Syllabus Checklist - ICT (0417)Melissa Li100% (1)
- Robot ReportDocument49 pagesRobot ReportJiya MakwanaPas encore d'évaluation
- Risk Management Under Covid 19 CPA KimeuDocument32 pagesRisk Management Under Covid 19 CPA KimeuREJAY89Pas encore d'évaluation
- Statutory Construction - Legal MaximsDocument5 pagesStatutory Construction - Legal MaximsglendaPas encore d'évaluation
- VRF Plus 2011 CatalogDocument32 pagesVRF Plus 2011 CatalogJorge DovalePas encore d'évaluation
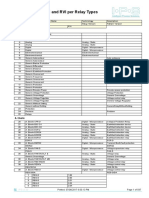
- IPS-ENERGY - Available Relay ModelsDocument597 pagesIPS-ENERGY - Available Relay Modelsbrahim100% (2)
- Factors Affecting Cultural Foods PlanningDocument8 pagesFactors Affecting Cultural Foods PlanningRegie Atienza50% (4)
- Definition of Terms (Fire Code of The Philippines)Document9 pagesDefinition of Terms (Fire Code of The Philippines)broomer27Pas encore d'évaluation
- ECC Chemical Process Pumps GuideDocument84 pagesECC Chemical Process Pumps GuideIwan KurniawanPas encore d'évaluation
- Procedural Due Process - Refers To The Mode of Procedure Which GovernmentDocument13 pagesProcedural Due Process - Refers To The Mode of Procedure Which GovernmentCharlene M. GalenzogaPas encore d'évaluation
- Streeter v. Secretary, Department of Corrections Et Al - Document No. 3Document2 pagesStreeter v. Secretary, Department of Corrections Et Al - Document No. 3Justia.comPas encore d'évaluation
- Rig 2017Document34 pagesRig 2017ralphPas encore d'évaluation
- Wattyl Killrust Brochure 2Document6 pagesWattyl Killrust Brochure 2Tech 84Pas encore d'évaluation
- Dashboard - Harare PolytechnicDocument4 pagesDashboard - Harare PolytechnicTeewyz MarPas encore d'évaluation
- Get That JobDocument12 pagesGet That JobNguyen PhamPas encore d'évaluation
- Introduction to ShipbuildingDocument7 pagesIntroduction to Shipbuildingmanoj narayananPas encore d'évaluation
- Delivering Success Tesco Case Study On BSCDocument4 pagesDelivering Success Tesco Case Study On BSCWenuri KasturiarachchiPas encore d'évaluation
- MS E-603 07/21_V1 High Performance Epoxy CoatingDocument1 pageMS E-603 07/21_V1 High Performance Epoxy CoatingchengkkPas encore d'évaluation
- To Compare The Efficacy, Safety and Cost - Effectiveness of Two Different Antisnake Venom Formulations (Antisnake Venom Powder and Antisnake Venom Liquid) at DHQ Hospital BadinDocument5 pagesTo Compare The Efficacy, Safety and Cost - Effectiveness of Two Different Antisnake Venom Formulations (Antisnake Venom Powder and Antisnake Venom Liquid) at DHQ Hospital BadinInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- RRV DC: 3.54 In. (90 MM)Document7 pagesRRV DC: 3.54 In. (90 MM)Trevor AdamsPas encore d'évaluation