Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- BattleRope Ebook FinalDocument38 pagesBattleRope Ebook FinalAnthony Dinicolantonio100% (1)
- A Financial History of The United States PDFDocument398 pagesA Financial History of The United States PDFiztok_ropotar6022Pas encore d'évaluation
- Asymetry Analysis of Breast Thermograma Using Automated SegmentationDocument8 pagesAsymetry Analysis of Breast Thermograma Using Automated Segmentationazazel17Pas encore d'évaluation
- APARICIO Frances Et Al. (Eds.) - Musical Migrations Transnationalism and Cultural Hybridity in Latino AmericaDocument218 pagesAPARICIO Frances Et Al. (Eds.) - Musical Migrations Transnationalism and Cultural Hybridity in Latino AmericaManuel Suzarte MarinPas encore d'évaluation
- Teaching Philosophy StatementDocument25 pagesTeaching Philosophy Statementtchrdale27Pas encore d'évaluation
- Modern Prometheus Editing The HumanDocument399 pagesModern Prometheus Editing The HumanHARTK 70Pas encore d'évaluation
- Ila 0306Document11 pagesIla 0306Hong ChenPas encore d'évaluation
- He Didnt Die in Vain - Take No GloryDocument2 pagesHe Didnt Die in Vain - Take No GloryDagaerag Law OfficePas encore d'évaluation
- Hinog vs. MellicorDocument11 pagesHinog vs. MellicorGreta VilarPas encore d'évaluation
- Computer Literacy Skills and Self-Efficacy Among Grade-12 - Computer System Servicing (CSS) StudentsDocument25 pagesComputer Literacy Skills and Self-Efficacy Among Grade-12 - Computer System Servicing (CSS) StudentsNiwre Gumangan AguiwasPas encore d'évaluation
- Module 4 Business EthicsDocument4 pagesModule 4 Business EthicsddddddaaaaeeeePas encore d'évaluation
- Lolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad MedinaceliDocument3 pagesLolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad Medinacelichatmche-06Pas encore d'évaluation
- Barclays Global FX Quarterly Fed On Hold Eyes On GrowthDocument42 pagesBarclays Global FX Quarterly Fed On Hold Eyes On GrowthgneymanPas encore d'évaluation
- Apr 00Document32 pagesApr 00nanda2006bPas encore d'évaluation
- Another Monster - Chapter 5 - Kinderheim 511Document7 pagesAnother Monster - Chapter 5 - Kinderheim 511Jaime MontoyaPas encore d'évaluation
- Heart Rate Variability - Wikipedia PDFDocument30 pagesHeart Rate Variability - Wikipedia PDFLevon HovhannisyanPas encore d'évaluation
- Solution Manual For Management A Focus On Leaders Plus 2014 Mymanagementlab With Pearson Etext Package 2 e Annie MckeeDocument24 pagesSolution Manual For Management A Focus On Leaders Plus 2014 Mymanagementlab With Pearson Etext Package 2 e Annie MckeeAnnGregoryDDSemcxo100% (90)
- Appendix I Leadership Questionnaire: Ior Description Questionnaire (LBDQ - Form XII 1962) - The Division IntoDocument24 pagesAppendix I Leadership Questionnaire: Ior Description Questionnaire (LBDQ - Form XII 1962) - The Division IntoJoan GonzalesPas encore d'évaluation
- Examination of Conscience Ten Commandments PDFDocument2 pagesExamination of Conscience Ten Commandments PDFAntonioPas encore d'évaluation
- NCLEX 20QUESTIONS 20safety 20and 20infection 20controlDocument8 pagesNCLEX 20QUESTIONS 20safety 20and 20infection 20controlCassey MillanPas encore d'évaluation
- A Week in My CountryDocument2 pagesA Week in My CountryAQhuewulland Youngprincess HokageNarutoPas encore d'évaluation
- 9 - Digest - Mari Vs BonillaDocument2 pages9 - Digest - Mari Vs BonillaMarivic Escueta100% (1)
- Mark Scheme Big Cat FactsDocument3 pagesMark Scheme Big Cat FactsHuyền MyPas encore d'évaluation
- The Endless Pursuit of Truth: Subalternity and Marginalization in Post-Neorealist Italian FilmDocument206 pagesThe Endless Pursuit of Truth: Subalternity and Marginalization in Post-Neorealist Italian FilmPaul MathewPas encore d'évaluation
- Graduation Ceremony 2013Document7 pagesGraduation Ceremony 2013Angelie Hermoso RoldanPas encore d'évaluation
- Operations Management and Operations PerformanceDocument59 pagesOperations Management and Operations PerformancePauline LagtoPas encore d'évaluation
- Of Bones and Buddhas Contemplation of TH PDFDocument215 pagesOf Bones and Buddhas Contemplation of TH PDFCPas encore d'évaluation
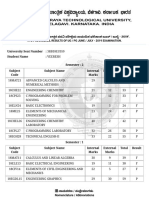
- VTU Result PDFDocument2 pagesVTU Result PDFVaibhavPas encore d'évaluation
- Contents:: Project ProgressDocument22 pagesContents:: Project ProgressJosé VicentePas encore d'évaluation
- Network Firewall SecurityDocument133 pagesNetwork Firewall Securitysagar323Pas encore d'évaluation