Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elliot Hulse - Rational Fasting Diet ManualDocument43 pagesElliot Hulse - Rational Fasting Diet ManualRyan Franco96% (27)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Sothys, The Professional DifferenceDocument29 pagesSothys, The Professional DifferenceNazihCosmeticsPas encore d'évaluation
- Raphanus Raphanistrum Subsp. Sativus: Scientifi C Name FamilyDocument41 pagesRaphanus Raphanistrum Subsp. Sativus: Scientifi C Name FamilyAlmas TPas encore d'évaluation
- Reviewon Cervical CancerDocument7 pagesReviewon Cervical CancerAlmas TPas encore d'évaluation
- 1007 Stem Cell Resourse Edition3 PDFDocument56 pages1007 Stem Cell Resourse Edition3 PDFNila astutiPas encore d'évaluation
- Poorolajal 2016Document7 pagesPoorolajal 2016Almas TPas encore d'évaluation
- Total Phenolic and Flavonoid Contents and Antioxidant Activities of Two Raphanus Sativus L. Cultivars (Cherry Belle and Valentine)Document6 pagesTotal Phenolic and Flavonoid Contents and Antioxidant Activities of Two Raphanus Sativus L. Cultivars (Cherry Belle and Valentine)Almas TPas encore d'évaluation
- D070415 PDFDocument5 pagesD070415 PDFRosyid PrasetyoPas encore d'évaluation
- Diabetes Mellitus: A Review On Pathophysiology, Current Status of Oral Medications and Future PerspectivesDocument22 pagesDiabetes Mellitus: A Review On Pathophysiology, Current Status of Oral Medications and Future PerspectivesAlmas TPas encore d'évaluation
- Raphanus Raphanistrum Subsp. Sativus: Scientifi C Name FamilyDocument41 pagesRaphanus Raphanistrum Subsp. Sativus: Scientifi C Name FamilyAlmas TPas encore d'évaluation
- Diarrhoeal Disease WhoDocument3 pagesDiarrhoeal Disease WhoAlmas TPas encore d'évaluation
- Total Phenolic and Flavonoid Contents and Antioxidant Activities of Two Raphanus Sativus L. Cultivars (Cherry Belle and Valentine)Document6 pagesTotal Phenolic and Flavonoid Contents and Antioxidant Activities of Two Raphanus Sativus L. Cultivars (Cherry Belle and Valentine)Almas TPas encore d'évaluation
- Diabetes Mellitus: A Review On Pathophysiology, Current Status of Oral Medications and Future PerspectivesDocument22 pagesDiabetes Mellitus: A Review On Pathophysiology, Current Status of Oral Medications and Future PerspectivesAlmas TPas encore d'évaluation
- Raphanus Raphanistrum Subsp. Sativus: Scientifi C Name FamilyDocument41 pagesRaphanus Raphanistrum Subsp. Sativus: Scientifi C Name FamilyAlmas TPas encore d'évaluation
- Streptozotocin, Type I Diabetes Severity and Bone: Katherine Motyl and Laura R. MccabeDocument20 pagesStreptozotocin, Type I Diabetes Severity and Bone: Katherine Motyl and Laura R. MccabeAlmas TPas encore d'évaluation
- Diabetes Mellitus: A Review On Pathophysiology, Current Status of Oral Medications and Future PerspectivesDocument22 pagesDiabetes Mellitus: A Review On Pathophysiology, Current Status of Oral Medications and Future PerspectivesAlmas TPas encore d'évaluation
- Total Phenolic and Flavonoid Contents and Antioxidant Activities of Two Raphanus Sativus L. Cultivars (Cherry Belle and Valentine)Document6 pagesTotal Phenolic and Flavonoid Contents and Antioxidant Activities of Two Raphanus Sativus L. Cultivars (Cherry Belle and Valentine)Almas TPas encore d'évaluation
- Visual and Auditori Young Old PDFDocument2 pagesVisual and Auditori Young Old PDFAlmas TPas encore d'évaluation
- Free Radical Biology & Medicine: Justin L. Rains, Sushil K. JainDocument9 pagesFree Radical Biology & Medicine: Justin L. Rains, Sushil K. JainAlmas TPas encore d'évaluation
- Art:10.1186/s13728 014 0020 7Document7 pagesArt:10.1186/s13728 014 0020 7Almas TPas encore d'évaluation
- Influence of Mast Cells On Dengue Protective Immunity and Immune PathologyDocument5 pagesInfluence of Mast Cells On Dengue Protective Immunity and Immune PathologyAlmas TPas encore d'évaluation
- Rizki - Amalia - Faktor Faktor Perbesaran Prostat PDFDocument8 pagesRizki - Amalia - Faktor Faktor Perbesaran Prostat PDFAlmas TPas encore d'évaluation
- 10 1152@ajprenal 00559 2015Document10 pages10 1152@ajprenal 00559 2015Almas TPas encore d'évaluation
- Diarrhoeal Disease WhoDocument3 pagesDiarrhoeal Disease WhoAlmas TPas encore d'évaluation
- Malformation of The KidneyDocument18 pagesMalformation of The KidneyAlmas TPas encore d'évaluation
- Gonzalez2015 PDFDocument10 pagesGonzalez2015 PDFAlmas TPas encore d'évaluation
- Gonzalez2015 PDFDocument10 pagesGonzalez2015 PDFAlmas TPas encore d'évaluation
- 10 1038@nrdp 2016 94Document17 pages10 1038@nrdp 2016 94Maya SwariPas encore d'évaluation
- Pathophys UrinalysisDocument9 pagesPathophys UrinalysisMohsen HaleemPas encore d'évaluation
- Hallows 2010Document11 pagesHallows 2010Almas TPas encore d'évaluation
- Protein Phosphatase 2C (PP2C) Is Responsible For VP-induced Dephosphorylation of AQP2 Serine 261Document40 pagesProtein Phosphatase 2C (PP2C) Is Responsible For VP-induced Dephosphorylation of AQP2 Serine 261Almas TPas encore d'évaluation
- Guzman 2015Document13 pagesGuzman 2015Almas TPas encore d'évaluation
- FD PDFDocument580 pagesFD PDFAinul LuthfiPas encore d'évaluation
- List of S-Phrases and R-PhrasesDocument7 pagesList of S-Phrases and R-PhrasesvanyshPas encore d'évaluation
- NAGC 0910 Tulsa Final BTDocument40 pagesNAGC 0910 Tulsa Final BTlparliPas encore d'évaluation
- Safety For LabDocument14 pagesSafety For LabAravind B PatilPas encore d'évaluation
- Yoga and Hyperthyroidism PDFDocument16 pagesYoga and Hyperthyroidism PDFRaushan Kumar MishraPas encore d'évaluation
- Read The Text and Answer Questions 5 and 6.: Cookbook. New York: DK Publishing, 2007, P. 8Document1 pageRead The Text and Answer Questions 5 and 6.: Cookbook. New York: DK Publishing, 2007, P. 8matheus gonçalvesPas encore d'évaluation
- Metode DQS ImunisasiDocument10 pagesMetode DQS ImunisasidianPas encore d'évaluation
- Global Developmental DelayDocument2 pagesGlobal Developmental DelayAtlerPas encore d'évaluation
- Passport XG Service ManualDocument544 pagesPassport XG Service ManualThatch50% (2)
- LCB ResponseDocument13 pagesLCB ResponseLas Vegas Review-JournalPas encore d'évaluation
- Pain Management: Dr. Prabowo Wicaksono Span Bagian/Smf Anestesi FK Unissula/Rsisa 2007Document27 pagesPain Management: Dr. Prabowo Wicaksono Span Bagian/Smf Anestesi FK Unissula/Rsisa 2007Fendy PrasetyoPas encore d'évaluation
- Top 50 Global Stem Cell InfluencersDocument25 pagesTop 50 Global Stem Cell InfluencersranasoftPas encore d'évaluation
- Abeba Final Thesis After DefenceDocument112 pagesAbeba Final Thesis After DefenceYayew MaruPas encore d'évaluation
- Mendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFDocument11 pagesMendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFJuan PalomoPas encore d'évaluation
- List of Instruments For 2nd Year BDSDocument17 pagesList of Instruments For 2nd Year BDSMohammad ShoebPas encore d'évaluation
- Prevencion DeliriumDocument13 pagesPrevencion DeliriumCarlos Hutarra DiazPas encore d'évaluation
- Post Retirement Medical Facilities Scheme (PRMFS) For Employees of D.S.I.I.Dc. Ltd. TitleDocument4 pagesPost Retirement Medical Facilities Scheme (PRMFS) For Employees of D.S.I.I.Dc. Ltd. Titleanand#99Pas encore d'évaluation
- Pediatric Neuropsychology: What Should I Expect?Document2 pagesPediatric Neuropsychology: What Should I Expect?Pradeep JNAPas encore d'évaluation
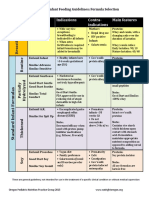
- Formula Selection OPNPGDocument2 pagesFormula Selection OPNPGRina PratiwiPas encore d'évaluation
- Magnesium Nitrate HexahydrateDocument4 pagesMagnesium Nitrate HexahydrateCarmen M AvinazarPas encore d'évaluation
- SPE GanjaDocument4 pagesSPE Ganjaintan kusumaningtyasPas encore d'évaluation
- Genetic Engineering Applications in Animal BreedingDocument6 pagesGenetic Engineering Applications in Animal BreedingFadilla HadiwijayaPas encore d'évaluation
- HHS Public AccessDocument16 pagesHHS Public AccessintanPas encore d'évaluation
- Immunology Mcqs-I (Gate Helpline)Document5 pagesImmunology Mcqs-I (Gate Helpline)Santhosh KalashPas encore d'évaluation
- Congestive Heart FailureDocument4 pagesCongestive Heart FailureEPas encore d'évaluation
- Alternative Treatment Strategies For Pseudo-Class III Malocclusion With Mild AsymmetryDocument17 pagesAlternative Treatment Strategies For Pseudo-Class III Malocclusion With Mild AsymmetrySchwan AbdulkareemPas encore d'évaluation
- Quantitative Estimation of Phytoconstituents of Caesalpinia PulcherrimaDocument5 pagesQuantitative Estimation of Phytoconstituents of Caesalpinia PulcherrimaSriArthiPas encore d'évaluation
- Vibrato Michael Trimble PDFDocument7 pagesVibrato Michael Trimble PDFCinqMars100% (1)