Vous aimerez peut-être aussi
- Hayashi Reiki ManualDocument14 pagesHayashi Reiki Manualboomerb100% (4)
- Tumours of The Adrenal GlandDocument34 pagesTumours of The Adrenal GlandSonam JoshiPas encore d'évaluation
- Telephone DirectoryDocument4 pagesTelephone DirectoryAnonymous QL0z40Fs9vPas encore d'évaluation
- Clinical Practice Guidelines - 2017Document54 pagesClinical Practice Guidelines - 2017Cem ÜnsalPas encore d'évaluation
- Pheochromocytoma in Genetic Disorders - UpToDateDocument11 pagesPheochromocytoma in Genetic Disorders - UpToDateLaura Marina IlincaPas encore d'évaluation
- SDL 10 BMS16091064Document5 pagesSDL 10 BMS16091064Jonathan YeohPas encore d'évaluation
- Pheochromocytoma - WikipediaDocument1 pagePheochromocytoma - WikipediaIulian GherasimPas encore d'évaluation
- The Endocrine System Path - Week 3Document11 pagesThe Endocrine System Path - Week 3joatasouzaPas encore d'évaluation
- Renal, Urinary Systems - ElectrolytesDocument692 pagesRenal, Urinary Systems - ElectrolytesRoshan MevadaPas encore d'évaluation
- Epidemiology, Natural History, Pathology and Management of Medulloblastoma in ChildrenDocument48 pagesEpidemiology, Natural History, Pathology and Management of Medulloblastoma in ChildrenSam OlukaPas encore d'évaluation
- 1 s2.0 S0085253815518541 MainDocument6 pages1 s2.0 S0085253815518541 MainaripPas encore d'évaluation
- Pituitary AdenomasDocument47 pagesPituitary AdenomasSabrina whtPas encore d'évaluation
- CA AdrenalDocument8 pagesCA AdrenalCleysser Antonio Custodio PolarPas encore d'évaluation
- Ent Mcqs For Part I Exam: Prepared By: Dr. Fouad ShamsanDocument86 pagesEnt Mcqs For Part I Exam: Prepared By: Dr. Fouad ShamsanAli QuwarahPas encore d'évaluation
- Pathology Aspect Pituitary Gland: By. Meike Rachmawati, DR Pathology Anatomy Department Medical Faculty-UnisbaDocument35 pagesPathology Aspect Pituitary Gland: By. Meike Rachmawati, DR Pathology Anatomy Department Medical Faculty-UnisbadeasyahPas encore d'évaluation
- Renal Cell Carcinoma in Young Patients: A Review of Recent LiteratureDocument6 pagesRenal Cell Carcinoma in Young Patients: A Review of Recent LiteratureSAhand HamzaPas encore d'évaluation
- Endocrine System PathologyDocument57 pagesEndocrine System PathologyCARSON 539Pas encore d'évaluation
- Ped Solid TumorDocument52 pagesPed Solid TumorIndranil GhoshPas encore d'évaluation
- Seminar: Jacques W M Lenders, Graeme Eisenhofer, Massimo Mannelli, Karel PacakDocument11 pagesSeminar: Jacques W M Lenders, Graeme Eisenhofer, Massimo Mannelli, Karel PacakAlexandru CozmaPas encore d'évaluation
- Pediatric Brain TumorDocument49 pagesPediatric Brain TumorJessica Victoria SudanawidjajaPas encore d'évaluation
- HHS Public Access: Pituitary TumorsDocument12 pagesHHS Public Access: Pituitary TumorsFauzi NoviaPas encore d'évaluation
- Neuropathologic Features of Central Nervous System HemangioblastomaDocument11 pagesNeuropathologic Features of Central Nervous System HemangioblastomaDavid Camilo GomezPas encore d'évaluation
- Rodgers Et Al-2012-British Journal of HaematologyDocument10 pagesRodgers Et Al-2012-British Journal of HaematologySalwiyadiPas encore d'évaluation
- Pathology of The Endocrine System: Causes A. Pituitary Usually Anterior LobeDocument19 pagesPathology of The Endocrine System: Causes A. Pituitary Usually Anterior LobecystanarisaPas encore d'évaluation
- 4.1c - MEN Syndromes - Nov.10 - Dr. GalangDocument2 pages4.1c - MEN Syndromes - Nov.10 - Dr. GalangMiel Raphael AranillaPas encore d'évaluation
- Path Lab Name: Onyedika Egbujo No: #671 Topic: PheochromocytomaDocument4 pagesPath Lab Name: Onyedika Egbujo No: #671 Topic: PheochromocytomaOnyedika EgbujoPas encore d'évaluation
- Tumors of The Nervous SystemDocument45 pagesTumors of The Nervous SystemIsaac MwangiPas encore d'évaluation
- Parathyroid N AdrenalDocument3 pagesParathyroid N Adrenalvishalyadav5656Pas encore d'évaluation
- Small Round Cell TumorsDocument131 pagesSmall Round Cell TumorschinnnababuPas encore d'évaluation
- Sdxxxxy MRPDocument10 pagesSdxxxxy MRPnon_zensePas encore d'évaluation
- Thyroid Neoplasms: Muhammad Haris Aslam Janjua Resident, Surgical Unit I SIMS/Services Hospital, LahoreDocument116 pagesThyroid Neoplasms: Muhammad Haris Aslam Janjua Resident, Surgical Unit I SIMS/Services Hospital, LahoreHajra IsrarPas encore d'évaluation
- Thyroid: Cytopathology and Its Histopathological BasesDocument49 pagesThyroid: Cytopathology and Its Histopathological BasesYuli Setio Budi PrabowoPas encore d'évaluation
- PheochromocytomaDocument5 pagesPheochromocytomahussain AltaherPas encore d'évaluation
- Basic Science Notes MRCP AssDocument9 pagesBasic Science Notes MRCP AssUm HamoOdPas encore d'évaluation
- 2 Tumour Biology and Histopathology of Neuroendocrine TumoursDocument17 pages2 Tumour Biology and Histopathology of Neuroendocrine TumoursUvi Cancino RamosPas encore d'évaluation
- Patologi Endokrin 2016Document132 pagesPatologi Endokrin 2016agusPas encore d'évaluation
- Patho Prelim 2nd SemDocument14 pagesPatho Prelim 2nd SemIC BPas encore d'évaluation
- 2-Adrenal Path.Document72 pages2-Adrenal Path.Lea MonzerPas encore d'évaluation
- Actualizaciones Oaragangliomas Sociedad EndocrinoDocument9 pagesActualizaciones Oaragangliomas Sociedad EndocrinoCharly FlowPas encore d'évaluation
- FeocromocitomaDocument15 pagesFeocromocitomaRaul GascueñaPas encore d'évaluation
- Teratoma TranslateDocument4 pagesTeratoma TranslateHr. EmhyPas encore d'évaluation
- 2 The Nature of HNSCC-WayanS, DRSPBDocument29 pages2 The Nature of HNSCC-WayanS, DRSPBLeise Kestia Rosalyn LimpelehPas encore d'évaluation
- Leukemias & Lymphomas - HY USMLEDocument87 pagesLeukemias & Lymphomas - HY USMLEMatt McGlothlinPas encore d'évaluation
- Pheochromocytoma and Paraganglioma: A Review of Diagnosis, Management and Treatment of Rare Causes of HypertensionDocument6 pagesPheochromocytoma and Paraganglioma: A Review of Diagnosis, Management and Treatment of Rare Causes of HypertensionBernaHerediaPas encore d'évaluation
- MRCP Notes 2006Document117 pagesMRCP Notes 2006Walaa Ismail HidirbiPas encore d'évaluation
- Retinal Hemangiomas - American Academy of OphthalmologyDocument10 pagesRetinal Hemangiomas - American Academy of OphthalmologyLydia Angelia YanitaPas encore d'évaluation
- Mitochondrial Encephalomyopathies (MEM)Document66 pagesMitochondrial Encephalomyopathies (MEM)Fatma KaledPas encore d'évaluation
- Head and Neck: Salivary Gland Tumors: An OverviewDocument12 pagesHead and Neck: Salivary Gland Tumors: An OverviewVanessa MordiPas encore d'évaluation
- Malignant Pheochromocytoma - A Diagnostic and Therapeutic DilemmaDocument5 pagesMalignant Pheochromocytoma - A Diagnostic and Therapeutic DilemmaJad DegheiliPas encore d'évaluation
- Neoplasms Thyroid N ParathyroidsDocument88 pagesNeoplasms Thyroid N ParathyroidsBkas GrgPas encore d'évaluation
- Hemostasis - Hematology BlockDocument40 pagesHemostasis - Hematology BlockamandaPas encore d'évaluation
- 15c MedullaryThyroidCancer-ITSBookChapterDocument10 pages15c MedullaryThyroidCancer-ITSBookChapterIulia JulyPas encore d'évaluation
- Management of Paraproteinaemia: ReviewDocument7 pagesManagement of Paraproteinaemia: ReviewInaGargPas encore d'évaluation
- Brain TumoursDocument25 pagesBrain Tumoursmulumbamusonda25Pas encore d'évaluation
- Paraneoplastic SyndromesDocument15 pagesParaneoplastic SyndromesironPas encore d'évaluation
- B17M4L4B PheochromocytomaDocument6 pagesB17M4L4B PheochromocytomaJoaquim RodriguezPas encore d'évaluation
- Duchenne Muscular DystrophyDocument10 pagesDuchenne Muscular DystrophyZeeshan KhanPas encore d'évaluation
- The Dysmyelopoietic DisordersDocument26 pagesThe Dysmyelopoietic DisordersJoseph FronterasPas encore d'évaluation
- Pituitary Apoplexy Pathophysiology Diagnosis and MDocument6 pagesPituitary Apoplexy Pathophysiology Diagnosis and MlathifatulPas encore d'évaluation
- Path Prep - GeoffDocument98 pagesPath Prep - GeoffVerlyn YtPas encore d'évaluation
- Fast Facts: Myelofibrosis: Reviewed by Professor Ruben A. MesaD'EverandFast Facts: Myelofibrosis: Reviewed by Professor Ruben A. MesaPas encore d'évaluation
- Neuroendocrine Tumors: Surgical Evaluation and ManagementD'EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydPas encore d'évaluation
- Pheochromocytomas, Paragangliomas and Disorders of the Sympathoadrenal System: Clinical Features, Diagnosis and ManagementD'EverandPheochromocytomas, Paragangliomas and Disorders of the Sympathoadrenal System: Clinical Features, Diagnosis and ManagementLewis LandsbergPas encore d'évaluation
- Corneal Degeneration: By-Shweta Santosh Maurya 2 Year B. Optometry Institute For Technology and ManagementDocument43 pagesCorneal Degeneration: By-Shweta Santosh Maurya 2 Year B. Optometry Institute For Technology and ManagementTaro RahmatiaPas encore d'évaluation
- Jve 2 27Document5 pagesJve 2 27Taro RahmatiaPas encore d'évaluation
- Potensi Cabai Sebagai Anti-Aterosklerosis: Fakultas Kedokteran Universitas LampungDocument6 pagesPotensi Cabai Sebagai Anti-Aterosklerosis: Fakultas Kedokteran Universitas LampungTaro RahmatiaPas encore d'évaluation
- Journal Reading DR Arief DADocument26 pagesJournal Reading DR Arief DATaro RahmatiaPas encore d'évaluation
- Basic Musculoskeletal Radiologic InterpretationDocument2 pagesBasic Musculoskeletal Radiologic InterpretationTaro RahmatiaPas encore d'évaluation
- Arthropod BitesDocument60 pagesArthropod BitesTaro RahmatiaPas encore d'évaluation
- Treatment Using Ethanolic Extract of Cocoa Beans)Document5 pagesTreatment Using Ethanolic Extract of Cocoa Beans)Hidayah HarahapPas encore d'évaluation
- Ukuran BurnazinDocument2 pagesUkuran BurnazinTaro RahmatiaPas encore d'évaluation
- Namdaemun Market Location:: Exit From Line 4 - Hoehyeon StationDocument3 pagesNamdaemun Market Location:: Exit From Line 4 - Hoehyeon StationTaro RahmatiaPas encore d'évaluation
- Abdul RohimDocument1 pageAbdul RohimTaro RahmatiaPas encore d'évaluation
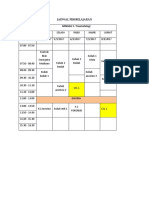
- Jadwal Minggu I Blok EmergencyDocument1 pageJadwal Minggu I Blok EmergencyTaro RahmatiaPas encore d'évaluation
- Penilaian Konsumsi Food Recall NikenDocument3 pagesPenilaian Konsumsi Food Recall NikenTaro RahmatiaPas encore d'évaluation
- Qwertyuiop LatihannnnDocument2 pagesQwertyuiop LatihannnnTaro RahmatiaPas encore d'évaluation
- Niken ByssinosisDocument23 pagesNiken ByssinosisTaro RahmatiaPas encore d'évaluation
- Pesticide Illness: Recognition, Diagnosis, ManagementDocument31 pagesPesticide Illness: Recognition, Diagnosis, Managementكسلان اكتب اسميPas encore d'évaluation
- Viral Skin InfectionDocument23 pagesViral Skin InfectionTaro RahmatiaPas encore d'évaluation
- Review Article: The Use of Stem Cells in Burn Wound Healing: A ReviewDocument9 pagesReview Article: The Use of Stem Cells in Burn Wound Healing: A ReviewTaro RahmatiaPas encore d'évaluation
- Pesticide PoisoningDocument34 pagesPesticide PoisoningappealingashishPas encore d'évaluation
- Facial Fractures: Sylvia Aparicio Harvard Medical School Year IVDocument0 pageFacial Fractures: Sylvia Aparicio Harvard Medical School Year IVRumah Kost Kontrakan AntapaniPas encore d'évaluation
- 22 Varicella Pink BookDocument24 pages22 Varicella Pink BookMohamad Syaikhul IslamPas encore d'évaluation
- Chronic Bronchitis in West Sweden A Matter of Smoking and Social ClassDocument10 pagesChronic Bronchitis in West Sweden A Matter of Smoking and Social ClassTaro RahmatiaPas encore d'évaluation
- Facial Fractures: Sylvia Aparicio Harvard Medical School Year IVDocument0 pageFacial Fractures: Sylvia Aparicio Harvard Medical School Year IVRumah Kost Kontrakan AntapaniPas encore d'évaluation
- Herbicide and Fungicide Toxicology 2014Document34 pagesHerbicide and Fungicide Toxicology 2014Taro RahmatiaPas encore d'évaluation
- 22 Varicella Pink BookDocument24 pages22 Varicella Pink BookMohamad Syaikhul IslamPas encore d'évaluation
- 2016 Article 111Document8 pages2016 Article 111Taro RahmatiaPas encore d'évaluation
- Facial Fractures: Sylvia Aparicio Harvard Medical School Year IVDocument0 pageFacial Fractures: Sylvia Aparicio Harvard Medical School Year IVRumah Kost Kontrakan AntapaniPas encore d'évaluation
- Family Eco Map Bapak ZulkiDocument1 pageFamily Eco Map Bapak ZulkiTaro RahmatiaPas encore d'évaluation
- Learning Objectives: Niken Rahmatia 1418011152Document17 pagesLearning Objectives: Niken Rahmatia 1418011152Taro RahmatiaPas encore d'évaluation
- Cushing SyndromeDocument17 pagesCushing SyndromeTaro RahmatiaPas encore d'évaluation
- Clinical Session Adult I-1 3Document34 pagesClinical Session Adult I-1 3Juan LinPas encore d'évaluation
- Respiratory PhysiologyDocument9 pagesRespiratory PhysiologyBrent TorresPas encore d'évaluation
- Modul Normal Delivery 2016Document8 pagesModul Normal Delivery 2016Alvin FarhanPas encore d'évaluation
- Immunization Schedule in India 2017 (Latest !!)Document13 pagesImmunization Schedule in India 2017 (Latest !!)rajPas encore d'évaluation
- HSG PresentationDocument18 pagesHSG Presentationashikin92Pas encore d'évaluation
- TELECARDIOLOGYDocument11 pagesTELECARDIOLOGYNancy Prasad100% (1)
- Basic and Clinical Pharmacology 12th Edition-Bertram Katzung Susan Masters Anthony Trevor-290-296 PDFDocument7 pagesBasic and Clinical Pharmacology 12th Edition-Bertram Katzung Susan Masters Anthony Trevor-290-296 PDFalinamatei1000000Pas encore d'évaluation
- Case StudyDocument4 pagesCase StudyTariq shahPas encore d'évaluation
- PALS Skills ChecklistDocument5 pagesPALS Skills ChecklistGiulia MeniconziPas encore d'évaluation
- 1.1.4.B ConcentrationDocument3 pages1.1.4.B ConcentrationAnonymous lFgKXClH0% (1)
- Indian Perspective For Probiotics: A Review: ArticleDocument12 pagesIndian Perspective For Probiotics: A Review: ArticleMurali DathanPas encore d'évaluation
- Dementia - StatPearls - NCBI BookshelfDocument7 pagesDementia - StatPearls - NCBI BookshelfSMA N 1 TOROHPas encore d'évaluation
- Epidemiology, Prevention and Control of Dengue: DR Tahira JaffarDocument36 pagesEpidemiology, Prevention and Control of Dengue: DR Tahira JaffarRaza UzuPas encore d'évaluation
- Case Study 103Document8 pagesCase Study 103Jonah MaasinPas encore d'évaluation
- Norethisterone JournalDocument29 pagesNorethisterone JournalAditya Syah PutraPas encore d'évaluation
- IPT Students - Non-Hospital Based Specialists KUANTANDocument113 pagesIPT Students - Non-Hospital Based Specialists KUANTANFatin nadhirah Kamaludin latifiPas encore d'évaluation
- Pathology MnemonicsDocument27 pagesPathology MnemonicsdyaPas encore d'évaluation
- 4 EL Husseinys Essentials of Cardiovascular System @eduwaves360Document236 pages4 EL Husseinys Essentials of Cardiovascular System @eduwaves360ahmed_abu_alrobPas encore d'évaluation
- EzhilDocument92 pagesEzhilRachitha GuttaPas encore d'évaluation
- Haemostasis: 1. Vascular SpasmDocument5 pagesHaemostasis: 1. Vascular SpasmAnurag YadavPas encore d'évaluation
- Brief Intervention: Mhgap-Ig Base Course - Field Test Version 1.00 - May 2012 1Document16 pagesBrief Intervention: Mhgap-Ig Base Course - Field Test Version 1.00 - May 2012 1TEOFILO PALSIMON JR.Pas encore d'évaluation
- Teleradiologi: Cross Reporting & Smart AssignDocument17 pagesTeleradiologi: Cross Reporting & Smart Assignrafael100% (1)
- 0 - Review of Post Graduate Medical Entrance Examination (PGMEE) (AAA) (PDFDrive - Com) Export PDFDocument39 pages0 - Review of Post Graduate Medical Entrance Examination (PGMEE) (AAA) (PDFDrive - Com) Export PDFAbu ÂwŞmž100% (2)
- All India Institute of Medical Sciences: List of Faculty - Departmentswise As On 10.10.2014 at The A.I.I.M.S., New DelhiDocument23 pagesAll India Institute of Medical Sciences: List of Faculty - Departmentswise As On 10.10.2014 at The A.I.I.M.S., New DelhiSaif AliPas encore d'évaluation
- Microbiological Quality of Non-SterileDocument5 pagesMicrobiological Quality of Non-SterilePaula BelloPas encore d'évaluation
- Chemical Peel Guidelines PDFDocument1 pageChemical Peel Guidelines PDFHasan MurdimanPas encore d'évaluation
- Photodiagnosis and Photodynamic Therapy: Case ReportDocument2 pagesPhotodiagnosis and Photodynamic Therapy: Case ReportMedPas encore d'évaluation