Vous aimerez peut-être aussi
- TugasDocument19 pagesTugasaaPas encore d'évaluation
- Carotid ESVS 2018Document79 pagesCarotid ESVS 2018Ahmed ElmallahPas encore d'évaluation
- Medical treatment and operative repair of abdominal aortic aneurysmsD'EverandMedical treatment and operative repair of abdominal aortic aneurysmsPas encore d'évaluation
- The Intensive Care Unit MaualDocument356 pagesThe Intensive Care Unit MaualMariefel Villanueva AlejagaPas encore d'évaluation
- Nicu ProtocolsDocument111 pagesNicu ProtocolsJoão Paulo PatoPas encore d'évaluation
- Autoimmune Hepatitis, Overlap Syndrome, Primary Sclerosing Cholangitis and Primary Biliary Cirrhosis in Clinical PracticeD'EverandAutoimmune Hepatitis, Overlap Syndrome, Primary Sclerosing Cholangitis and Primary Biliary Cirrhosis in Clinical PracticePas encore d'évaluation
- CDI22 Desk ReferenceDocument14 pagesCDI22 Desk ReferenceBanin AbadiPas encore d'évaluation
- Uti in WomanDocument6 pagesUti in WomanPrimasari DiahPas encore d'évaluation
- Murillo de Oliveira Antunes 2020Document15 pagesMurillo de Oliveira Antunes 2020Asisten Lab TLPPas encore d'évaluation
- Childhood MedulloblastmaDocument17 pagesChildhood MedulloblastmaIrenaPas encore d'évaluation
- Atherosclerosis: Naishi Li, Jingyuan Fu, Debby P. Koonen, Jan Albert Kuivenhoven, Harold Snieder, Marten H. HofkerDocument9 pagesAtherosclerosis: Naishi Li, Jingyuan Fu, Debby P. Koonen, Jan Albert Kuivenhoven, Harold Snieder, Marten H. HofkerdwirosidPas encore d'évaluation
- Deficiencies of the Urea Cycle - Clinical Significance and TherapyD'EverandDeficiencies of the Urea Cycle - Clinical Significance and TherapyPas encore d'évaluation
- Ecls GuidDocument24 pagesEcls GuidHanafieHeluthPas encore d'évaluation
- Retention and Selectivity in Liquid Chromatography: Prediction, Standardisation and Phase ComparisonsD'EverandRetention and Selectivity in Liquid Chromatography: Prediction, Standardisation and Phase ComparisonsPas encore d'évaluation
- ICU HandbookDocument146 pagesICU HandbookBulent InanPas encore d'évaluation
- Acute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionD'EverandAcute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionPas encore d'évaluation
- Basic First AidDocument53 pagesBasic First Aidlead_chipmunkPas encore d'évaluation
- Iron Deficiency and Anaemia in Women in the Gynaecological and Obstetrical Practice (with Case Reports)D'EverandIron Deficiency and Anaemia in Women in the Gynaecological and Obstetrical Practice (with Case Reports)Pas encore d'évaluation
- The Intensive Care Unit at The Mid Yorkshire Hospitals NHS TrustDocument164 pagesThe Intensive Care Unit at The Mid Yorkshire Hospitals NHS TrustRajiv Srinivasa71% (7)
- ESVS Thoracic Ds PDFDocument49 pagesESVS Thoracic Ds PDFFredy CarolPas encore d'évaluation
- Medical Signal CodeDocument30 pagesMedical Signal CodeAribbyan DhafinPas encore d'évaluation
- Ashi Bfa SH SampleDocument12 pagesAshi Bfa SH SampleDamien AshwoodPas encore d'évaluation
- A. Orlando Ortiz (Auth.) - Image-Guided Percutaneous Spine Biopsy-Springer International Publishing (2017)Document290 pagesA. Orlando Ortiz (Auth.) - Image-Guided Percutaneous Spine Biopsy-Springer International Publishing (2017)RUCHIR UTTAMPas encore d'évaluation
- 2023 CPG On The Management of Atherosclerotic Carotid and Vertebral Artery DiseaseDocument105 pages2023 CPG On The Management of Atherosclerotic Carotid and Vertebral Artery DiseaseElisa NovaesPas encore d'évaluation
- Icrp 94 Radiological ProtectionDocument84 pagesIcrp 94 Radiological ProtectionBudi ArifPas encore d'évaluation
- Secondary Brain Injury - Predicting and Preventing InsultsDocument8 pagesSecondary Brain Injury - Predicting and Preventing InsultsJavier Andrés Mora ArtéagaPas encore d'évaluation
- 1584 FemaDocument174 pages1584 Femamayor44patitoPas encore d'évaluation
- Optimized Supportive Care For Ebola Virus Disease: Clinical Management Standard Operating ProceduresDocument44 pagesOptimized Supportive Care For Ebola Virus Disease: Clinical Management Standard Operating ProceduresburhanPas encore d'évaluation
- AHA ACC Test Ergo Met RicoDocument56 pagesAHA ACC Test Ergo Met RicoValentina VaccaroPas encore d'évaluation
- Sorkin 1987Document50 pagesSorkin 1987Galuh EkaPas encore d'évaluation
- The Antioxidant and Anticancer Potentials of New Zealand Manuka Honey and Thyme HoneyDocument128 pagesThe Antioxidant and Anticancer Potentials of New Zealand Manuka Honey and Thyme Honeyمنير علي هباطيPas encore d'évaluation
- ''Sangrado Perioperatorio Severo GuiaDocument113 pages''Sangrado Perioperatorio Severo GuiaHECTOR ESTRADAPas encore d'évaluation
- Demicheli Et Al - 2000 - Prevention and Early Treatment of Influenza in Healthy AdultsDocument74 pagesDemicheli Et Al - 2000 - Prevention and Early Treatment of Influenza in Healthy AdultsМихаил РайцисPas encore d'évaluation
- CardiacDocument148 pagesCardiacadel husseinPas encore d'évaluation
- Human Factors in Air Transport Understanding Behavior and PerformanceDocument206 pagesHuman Factors in Air Transport Understanding Behavior and PerformanceKouda Hamza100% (2)
- MMS Internal Medicine Treatment & ProtocolsDocument248 pagesMMS Internal Medicine Treatment & ProtocolsVeselin PapazovPas encore d'évaluation
- Reabilitare Dupa AvcDocument91 pagesReabilitare Dupa AvcDiana StancaPas encore d'évaluation
- Contents in PrintDocument12 pagesContents in PrintkhojalkhelPas encore d'évaluation
- 203013DB TocDocument14 pages203013DB TocDeanna Marie MedequisoPas encore d'évaluation
- Asthama in ElderlyDocument72 pagesAsthama in ElderlyboyzonerajPas encore d'évaluation
- File, 3303, enDocument80 pagesFile, 3303, enshinichi kudoPas encore d'évaluation
- Quality of Life in Systemic SclerosisDocument10 pagesQuality of Life in Systemic SclerosisIsa RahmatikawatiPas encore d'évaluation
- Vol.13 Human Performance and LimitationsDocument222 pagesVol.13 Human Performance and LimitationsMostafa MohsenPas encore d'évaluation
- Otitis ExternaDocument166 pagesOtitis ExternaCarlos Rodríguez100% (2)
- Health Assessment 1Document6 pagesHealth Assessment 1Tejna KumariPas encore d'évaluation
- DHS Austere EMS Field GuideDocument298 pagesDHS Austere EMS Field GuideRicardo Luis Martin Sant'Anna100% (2)
- Chap 4Document92 pagesChap 4sandsphilipPas encore d'évaluation
- 2018 Book NursingInCriticalCareSetting PDFDocument532 pages2018 Book NursingInCriticalCareSetting PDFAnton HerdiansyahPas encore d'évaluation
- Endomorfin 2 PDFDocument36 pagesEndomorfin 2 PDFMuhammad Ichsan MustariPas encore d'évaluation
- Effectiveness of Homeopathy For Clinical Conditions - Evaluation of The Evidence PDFDocument301 pagesEffectiveness of Homeopathy For Clinical Conditions - Evaluation of The Evidence PDFYaniv AlgrablyPas encore d'évaluation
- JURCIC 888zuwen717z336ektk63in THDocument256 pagesJURCIC 888zuwen717z336ektk63in THManirarora EtiennePas encore d'évaluation
- Principles of Epidemiology in Public Health PracticeDocument512 pagesPrinciples of Epidemiology in Public Health PracticeAdare Oluwafemi Thomas100% (3)
- DL MX 94 AiimsDocument6 pagesDL MX 94 AiimsPramod N KPas encore d'évaluation
- Key Sensory PointsDocument2 pagesKey Sensory PointsPramod N KPas encore d'évaluation
- Short Segment Pedicle Screw Fixation of Thoracolumbar Fracture: A Case Series of 33 PatientsDocument8 pagesShort Segment Pedicle Screw Fixation of Thoracolumbar Fracture: A Case Series of 33 PatientsPramod N KPas encore d'évaluation
- DL ScoressssDocument8 pagesDL ScoressssPramod N KPas encore d'évaluation
- Management of Traumatic Thoracolumbar Fractures: A Systematic Review of The LiteratureDocument8 pagesManagement of Traumatic Thoracolumbar Fractures: A Systematic Review of The LiteratureAshraf AbbasPas encore d'évaluation
- Key Sensory PointsDocument6 pagesKey Sensory PointsJose Maria Dominguez RoldanPas encore d'évaluation
- Voccaro TLICS A-New-Classi cation-of-Thoracolumbar-Injuries PDFDocument9 pagesVoccaro TLICS A-New-Classi cation-of-Thoracolumbar-Injuries PDFPramod N KPas encore d'évaluation
- What Should An Ideal Spinal Injury Class PDFDocument12 pagesWhat Should An Ideal Spinal Injury Class PDFPramod N KPas encore d'évaluation
- DL TPSFDocument5 pagesDL TPSFPramod N KPas encore d'évaluation
- Thoracolumbar Vertebral Fractures in Sweden: An Analysis of 13,496 Patients Admitted To HospitalDocument8 pagesThoracolumbar Vertebral Fractures in Sweden: An Analysis of 13,496 Patients Admitted To HospitalPramod N KPas encore d'évaluation
- Stadhouder PDFDocument7 pagesStadhouder PDFPramod N KPas encore d'évaluation
- System (Cranial Mesh System) : Cranio Mesh 0.6Mm WXL Part No. Cranio Mesh 0.4Mm WXL Part NoDocument2 pagesSystem (Cranial Mesh System) : Cranio Mesh 0.6Mm WXL Part No. Cranio Mesh 0.4Mm WXL Part NoPramod N KPas encore d'évaluation
- Reverse and Pseudoreverse Cortical SignDocument6 pagesReverse and Pseudoreverse Cortical SignPramod N KPas encore d'évaluation
- Holdsworth PDFDocument15 pagesHoldsworth PDFPramod N KPas encore d'évaluation
- OsteomyelitisDocument29 pagesOsteomyelitisPramod N KPas encore d'évaluation
- BiomechanicalDocument3 pagesBiomechanicalPramod N KPas encore d'évaluation
- FR Santiago ClaasificnDocument13 pagesFR Santiago ClaasificnPramod N KPas encore d'évaluation
- Fracture HealingDocument11 pagesFracture HealingPramod N KPas encore d'évaluation
- TB Spine - Laboratory Diagnosis, Management of TB Spine Including MDR CasesDocument61 pagesTB Spine - Laboratory Diagnosis, Management of TB Spine Including MDR CasesPramod N KPas encore d'évaluation
- Ao Pedicle ScrewDocument3 pagesAo Pedicle ScrewPramod N KPas encore d'évaluation
- Cervical Traction 2Document13 pagesCervical Traction 2Dw Ipha Ma HaPas encore d'évaluation
- Telluride 2 Mis Spinal Fixation System Surgical TechniqueDocument32 pagesTelluride 2 Mis Spinal Fixation System Surgical TechniquePramod N KPas encore d'évaluation
- EnchondromaDocument1 pageEnchondromaPramod N KPas encore d'évaluation
- CDC 3Document12 pagesCDC 3Azmi FarhadiPas encore d'évaluation
- CA Vit D MetabolismDocument41 pagesCA Vit D MetabolismPramod N KPas encore d'évaluation
- Traditional Spinal InstrumentsDocument3 pagesTraditional Spinal InstrumentsPramod N KPas encore d'évaluation
- Bracing For Thoracolumbar FracturesDocument7 pagesBracing For Thoracolumbar FracturesPramod N KPas encore d'évaluation
- Cervical Traction 2Document13 pagesCervical Traction 2Dw Ipha Ma HaPas encore d'évaluation
- Reliability of HpeDocument2 pagesReliability of HpePramod N KPas encore d'évaluation
- 01MED1SET2017Document292 pages01MED1SET2017Elison CarvalhoPas encore d'évaluation
- 1 Introduction TraumaDocument14 pages1 Introduction TraumameirizameilyaniarmanPas encore d'évaluation
- Average Ambulance Response Times For 911 CallsDocument2 pagesAverage Ambulance Response Times For 911 CallsLindsey BasyePas encore d'évaluation
- Sweet Et Al. Systematic Review Clavicle and Rib FracturesDocument8 pagesSweet Et Al. Systematic Review Clavicle and Rib FracturesRut Herdianti P. EkasiwiPas encore d'évaluation
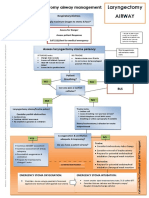
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementDocument1 pageLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IliePas encore d'évaluation
- PolytraumaDocument19 pagesPolytraumaSri MahadhanaPas encore d'évaluation
- ACLS Skills ChecklistDocument2 pagesACLS Skills ChecklistKary ParraPas encore d'évaluation
- National EMS Week 2019 InvitationDocument2 pagesNational EMS Week 2019 InvitationChris-Goldie LorezoPas encore d'évaluation
- Proposal For Ambulance Service For Camden, Hope, Lincolnville and RockportDocument20 pagesProposal For Ambulance Service For Camden, Hope, Lincolnville and RockportSpreading KnowledgePas encore d'évaluation
- 2020 Covid Deaths Ffs EmsDocument5 pages2020 Covid Deaths Ffs EmsepraetorianPas encore d'évaluation
- First Aid Sja Poster Emergency Adult e PDFDocument1 pageFirst Aid Sja Poster Emergency Adult e PDFKavinda BandaraPas encore d'évaluation
- AVPUDocument2 pagesAVPUAnissa Citra DewiPas encore d'évaluation
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDocument36 pagesProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoPas encore d'évaluation
- Terapi Oxygen Pada Pasien Covd-19Document24 pagesTerapi Oxygen Pada Pasien Covd-19normamPas encore d'évaluation
- Hafizah Hoshni PneumothoraxDocument47 pagesHafizah Hoshni PneumothoraxhafizahhoshniPas encore d'évaluation
- Emergency First Aid and CPRDocument15 pagesEmergency First Aid and CPRvhlactaotaoPas encore d'évaluation
- Situational Awareness TrainingDocument1 pageSituational Awareness TrainingFDRHPO North Country EMS Program AgencyPas encore d'évaluation
- DR - VP Singh - Medrecon (FINAL)Document45 pagesDR - VP Singh - Medrecon (FINAL)Virendar Pal SinghPas encore d'évaluation
- Advance Life SupportDocument198 pagesAdvance Life SupportPantelis PouliopoulosPas encore d'évaluation
- Fellowship Personal Statements ExamplesDocument57 pagesFellowship Personal Statements ExamplesFellowship Personal Statements Samples100% (11)
- Penawaran Permit Dan Paramedic Konser MLTRDocument1 pagePenawaran Permit Dan Paramedic Konser MLTRmantoumalemmalemPas encore d'évaluation
- Hospital Emergency Operations Plan TemplateDocument53 pagesHospital Emergency Operations Plan TemplateNicholaiCabadduPas encore d'évaluation
- EMS Systems in KoreaDocument4 pagesEMS Systems in KoreaJamison ParfittPas encore d'évaluation
- MCQ Trauma 2Document17 pagesMCQ Trauma 2sidra50% (4)
- First Responders Functions, Responsibilities and ProceduresDocument36 pagesFirst Responders Functions, Responsibilities and ProceduresDennis Esik MaligayaPas encore d'évaluation
- Trauma ATACC Manual 2014 PDFDocument460 pagesTrauma ATACC Manual 2014 PDFBenjamin Ng100% (1)
- Do Not Resuscitate Confirmation Form: To Direct The Practice of Paramedics and Firefighters After February 1, 2008Document2 pagesDo Not Resuscitate Confirmation Form: To Direct The Practice of Paramedics and Firefighters After February 1, 2008eschiuPas encore d'évaluation
- Research Study by UitmDocument24 pagesResearch Study by UitmMangayarkarasi ChandrakasanPas encore d'évaluation
- Neurological Assessment 1 - Assessing Level of ConsciousnessDocument1 pageNeurological Assessment 1 - Assessing Level of ConsciousnesskyawswakyawswaPas encore d'évaluation
- Core Clerkship GuideDocument18 pagesCore Clerkship GuideEduardo CésarPas encore d'évaluation
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!D'EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Évaluation : 5 sur 5 étoiles5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerD'EverandGut: the new and revised Sunday Times bestsellerÉvaluation : 4 sur 5 étoiles4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4 sur 5 étoiles4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryD'EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryÉvaluation : 4 sur 5 étoiles4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessD'EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisD'EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningD'EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningÉvaluation : 4 sur 5 étoiles4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)D'EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Évaluation : 4 sur 5 étoiles4/5 (378)
- To Explain the World: The Discovery of Modern ScienceD'EverandTo Explain the World: The Discovery of Modern ScienceÉvaluation : 3.5 sur 5 étoiles3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlD'EverandThe Marshmallow Test: Mastering Self-ControlÉvaluation : 4.5 sur 5 étoiles4.5/5 (58)