Vous aimerez peut-être aussi
- p2325 PDFDocument8 pagesp2325 PDFUtari UbPas encore d'évaluation
- IndianJCommunityMed 2016 41 2 154 173492 PDFDocument6 pagesIndianJCommunityMed 2016 41 2 154 173492 PDFUtari UbPas encore d'évaluation
- GOALSDocument1 pageGOALSUtari UbPas encore d'évaluation
- Mjms 16 2 004 PDFDocument6 pagesMjms 16 2 004 PDFUtari UbPas encore d'évaluation
- American Society of Hand Therapists Clinical Assessment RecommendationsDocument25 pagesAmerican Society of Hand Therapists Clinical Assessment RecommendationsUtari UbPas encore d'évaluation
- Penyamaan Persepsi TTG Pendekatan Holistik Komprehensif PDFDocument54 pagesPenyamaan Persepsi TTG Pendekatan Holistik Komprehensif PDFSyarifah FaihaaPas encore d'évaluation
- Cui 2012Document5 pagesCui 2012Utari UbPas encore d'évaluation
- Journal of Virology-2020-Wan-e02015-19.full PDFDocument15 pagesJournal of Virology-2020-Wan-e02015-19.full PDFUtari UbPas encore d'évaluation
- WHO - Haemoglobin Level For Anemia 2011Document6 pagesWHO - Haemoglobin Level For Anemia 2011Adhi SanjayaPas encore d'évaluation
- p2325 PDFDocument8 pagesp2325 PDFUtari UbPas encore d'évaluation
- The Prognostic Value of The Components of The Glasgow Coma Scale Following Acute StrokeDocument8 pagesThe Prognostic Value of The Components of The Glasgow Coma Scale Following Acute StrokeUtari UbPas encore d'évaluation
- American Society of Hand Therapists Clinical Assessment RecommendationsDocument25 pagesAmerican Society of Hand Therapists Clinical Assessment RecommendationsUtari UbPas encore d'évaluation
- Dementia Making Decisions PDFDocument68 pagesDementia Making Decisions PDFUtari UbPas encore d'évaluation
- Childhood and Adult Social Conditions and Risk of Stroke: Original PaperDocument8 pagesChildhood and Adult Social Conditions and Risk of Stroke: Original PaperUtari UbPas encore d'évaluation
- Impact of Supervision and Self-Assessment On Doctor-Patient Communication in Rural MexicoDocument9 pagesImpact of Supervision and Self-Assessment On Doctor-Patient Communication in Rural MexicoUtari UbPas encore d'évaluation
- Protocol PDFDocument29 pagesProtocol PDFUtari UbPas encore d'évaluation
- GOALSDocument1 pageGOALSUtari UbPas encore d'évaluation
- Protocol PDFDocument29 pagesProtocol PDFUtari UbPas encore d'évaluation
- Anthropometric Measurement of Patients Admitted To An Intensive Care Unit Jpcic 1000113 PDFDocument6 pagesAnthropometric Measurement of Patients Admitted To An Intensive Care Unit Jpcic 1000113 PDFAiya Auri GumantiPas encore d'évaluation
- Factors Predicting Length of Hospital Stay in Acute Stroke Patients PDFDocument5 pagesFactors Predicting Length of Hospital Stay in Acute Stroke Patients PDFUtari UbPas encore d'évaluation
- 0004 282X Anp 74 09 0718 PDFDocument5 pages0004 282X Anp 74 09 0718 PDFUtari UbPas encore d'évaluation
- GoalsDocument1 pageGoalsUtari UbPas encore d'évaluation
- The Reliability and Sensitivity of The National Institutes of Health Stroke Scale For Spontaneous Intracerebral Hemorrhage in An Uncontrolled SettingDocument4 pagesThe Reliability and Sensitivity of The National Institutes of Health Stroke Scale For Spontaneous Intracerebral Hemorrhage in An Uncontrolled SettingUtari UbPas encore d'évaluation
- A Prospective Study On The Prevalence and Risk Factors of Poststroke DepressionDocument13 pagesA Prospective Study On The Prevalence and Risk Factors of Poststroke DepressionUtari UbPas encore d'évaluation
- High Neutrophil-To-lymphocyte Ratio Is Associated With Increased Carotid ArteryDocument7 pagesHigh Neutrophil-To-lymphocyte Ratio Is Associated With Increased Carotid ArteryUtari UbPas encore d'évaluation
- Neutrophil Lymphocyte Ratios in Stroke Subtypes and Transient Ischemic AttackDocument5 pagesNeutrophil Lymphocyte Ratios in Stroke Subtypes and Transient Ischemic AttackUtari UbPas encore d'évaluation
- An Investigation Into The Relationship Between The Systemic Inflammatory Response and Survival A Glasgow Inflammation Outcome Study PDFDocument217 pagesAn Investigation Into The Relationship Between The Systemic Inflammatory Response and Survival A Glasgow Inflammation Outcome Study PDFUtari UbPas encore d'évaluation
- Preoperative Platelet-Lymphocyte Ratio Is Superior To Neutrophil-Lymphocyte Ratio As A Prognostic Factor For Soft-Tissue SarcomaDocument11 pagesPreoperative Platelet-Lymphocyte Ratio Is Superior To Neutrophil-Lymphocyte Ratio As A Prognostic Factor For Soft-Tissue SarcomaUtari UbPas encore d'évaluation
- Neutrophil To Lymphocyte Ratio at Admission Prognostic Factor in Patients With Acute Ischemic StrokeDocument7 pagesNeutrophil To Lymphocyte Ratio at Admission Prognostic Factor in Patients With Acute Ischemic StrokeUtari UbPas encore d'évaluation
- Inflammatory Biomarkers in Stroke and DementiaDocument117 pagesInflammatory Biomarkers in Stroke and DementiaUtari UbPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- CH 2 Atoms, Ions, and MoleculesDocument64 pagesCH 2 Atoms, Ions, and MoleculesBritney SimmsPas encore d'évaluation
- Assignment 1 Systems Analysis - EME5601Document7 pagesAssignment 1 Systems Analysis - EME5601Travis GrantPas encore d'évaluation
- The Effects of Oar-Shaft Stiffness andDocument9 pagesThe Effects of Oar-Shaft Stiffness andValentina DiamantePas encore d'évaluation
- Word Trek Lesson OutlinesDocument8 pagesWord Trek Lesson Outlinesapi-289048378Pas encore d'évaluation
- Aqua Mon 4000 PH Red Ox AnalyserDocument4 pagesAqua Mon 4000 PH Red Ox Analyserarvindgupta_2005Pas encore d'évaluation
- X Wing - Quick.referenceDocument6 pagesX Wing - Quick.referenceatilaT0RPas encore d'évaluation
- Error Codes (DTC) : 15 Electrical TroubleshootingDocument13 pagesError Codes (DTC) : 15 Electrical TroubleshootingPoyraz PoyrazPas encore d'évaluation
- Porphyria's Lover - Robert BrowningDocument9 pagesPorphyria's Lover - Robert Browningdearkatie6688Pas encore d'évaluation
- Sea Cucumber PDFDocument171 pagesSea Cucumber PDFRebeccaSulivanPas encore d'évaluation
- DCT PIR insulation technical data sheetDocument4 pagesDCT PIR insulation technical data sheetHenky MantophaniPas encore d'évaluation
- B. WoolworthsDocument5 pagesB. WoolworthsNjabulo Shakes NtuliPas encore d'évaluation
- Fischer Carbene Complexes in Organic SynthesisDocument9 pagesFischer Carbene Complexes in Organic SynthesisNorah AltayyarPas encore d'évaluation
- Answer Example Source Questio N Type Topic: Glish/Doanddoeshasandhave/Bjgd /post - HTMDocument92 pagesAnswer Example Source Questio N Type Topic: Glish/Doanddoeshasandhave/Bjgd /post - HTMFarhan HakimiPas encore d'évaluation
- TOPFLYtech Product - April 2023 - 4GDocument56 pagesTOPFLYtech Product - April 2023 - 4GmosorioPas encore d'évaluation
- In Situ Combustion: Amit Kumar Singh R270307004 Integrated (Ape) +mba (Uam) Semester: VIIIDocument17 pagesIn Situ Combustion: Amit Kumar Singh R270307004 Integrated (Ape) +mba (Uam) Semester: VIIISmita SharmaPas encore d'évaluation
- Din en 50155 (Vde 0115-200) - 2008-03Document42 pagesDin en 50155 (Vde 0115-200) - 2008-03Collins Akhimien100% (1)
- GRT9165 Product GuideDocument23 pagesGRT9165 Product GuideEslamAldenAbdoPas encore d'évaluation
- Caffeine Extraction 1 PDFDocument25 pagesCaffeine Extraction 1 PDFShanay ShahPas encore d'évaluation
- AmadeusDocument3 pagesAmadeusCleofe Mae Piñero AseñasPas encore d'évaluation
- Land Rover Range Rover Owners Manual 2007Document358 pagesLand Rover Range Rover Owners Manual 2007PetreCaracaleanu0% (1)
- Ahmed 2022Document20 pagesAhmed 2022Mariela Estefanía Marín LópezPas encore d'évaluation
- NPTEL Control Engineering Assignment 2 - SEO OptimizedDocument4 pagesNPTEL Control Engineering Assignment 2 - SEO OptimizedGanesh RadharamPas encore d'évaluation
- June 2023 BillingDocument10 pagesJune 2023 BillingEsther AkpanPas encore d'évaluation
- Enzymatic Browning and Its Prevention-American Chemical Society (1995)Document340 pagesEnzymatic Browning and Its Prevention-American Chemical Society (1995)danielguerinPas encore d'évaluation
- 3 1Document4 pages3 1HakanPas encore d'évaluation
- Steam TurbineDocument25 pagesSteam TurbineIshan JunejaPas encore d'évaluation
- Rom BlonDocument8 pagesRom BlonCharlesJustin AyunonPas encore d'évaluation
- FM200 Clean Agent System Installation GuideDocument6 pagesFM200 Clean Agent System Installation Guidehazro lizwan halimPas encore d'évaluation
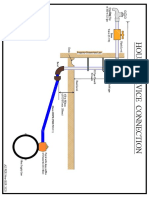
- House Service Connection NEW BSR 2020-1Document1 pageHouse Service Connection NEW BSR 2020-1Deshraj BairwaPas encore d'évaluation
- Civil Engineering Set 2Document13 pagesCivil Engineering Set 2Dev ThakurPas encore d'évaluation