Vous aimerez peut-être aussi
- PQM Quiz FinalDocument11 pagesPQM Quiz FinalSyeda Sadaf ZahraPas encore d'évaluation
- A Visual Rhetoric StudyDocument32 pagesA Visual Rhetoric StudylpettenkoferPas encore d'évaluation
- Sheiko 13week Beginner ProgramDocument16 pagesSheiko 13week Beginner ProgramAnders DahlPas encore d'évaluation
- Kidney Function Test-1Document11 pagesKidney Function Test-1jahansha kurramPas encore d'évaluation
- UrinalysisDocument10 pagesUrinalysisMichelle100% (2)
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case StudyPrincess Tindugan100% (1)
- Chapter 1: Introduction To Urinalysis: Urine CompositionDocument74 pagesChapter 1: Introduction To Urinalysis: Urine CompositionMegumi TadokoroPas encore d'évaluation
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case Study19lyon92100% (6)
- Estimation of Measurement Uncertainty For Electrical Conductivity in WaterDocument4 pagesEstimation of Measurement Uncertainty For Electrical Conductivity in WaterMaruthi KPas encore d'évaluation
- Physio 50qDocument70 pagesPhysio 50qAnonymous t5TDwd67% (3)
- Kumleben Commission ReportDocument232 pagesKumleben Commission ReportJulian Rademeyer100% (2)
- UKAYUNIK Chapter 1 To 12Document31 pagesUKAYUNIK Chapter 1 To 12Chiesa ArellanoPas encore d'évaluation
- Renal Function TestsDocument23 pagesRenal Function TestsKer YehunPas encore d'évaluation
- Blood Urea NitrogenDocument5 pagesBlood Urea NitrogenRachel Marie M. Gania0% (1)
- Toksik 2Document3 pagesToksik 2な ーPas encore d'évaluation
- Effects of Lactulose and Neomycin On Urea Metabolism in Cirrhotic SubjectsDocument5 pagesEffects of Lactulose and Neomycin On Urea Metabolism in Cirrhotic Subjectsnova adiPas encore d'évaluation
- Current Concepts of And: Hyperuricemia GoutDocument13 pagesCurrent Concepts of And: Hyperuricemia GoutAnonymous h0XxWy8SPas encore d'évaluation
- Uric AcidDocument6 pagesUric Acidmonday125100% (1)
- Treatment of Asymptomatic Hyperuricemia in Chronic Kidney DiseaseDocument4 pagesTreatment of Asymptomatic Hyperuricemia in Chronic Kidney DiseaseRonald Ariyanto WiradirnataPas encore d'évaluation
- Regulation of Uric Acid Metabolism and Excretion PDFDocument7 pagesRegulation of Uric Acid Metabolism and Excretion PDFYulanda YomemotoPas encore d'évaluation
- Uric Acid in Chronic Kidney Disease: CA Murakami, SM SozioDocument6 pagesUric Acid in Chronic Kidney Disease: CA Murakami, SM SozioHanny Friska YudistyawanPas encore d'évaluation
- Non-Protein Nitrogen CompoundsDocument6 pagesNon-Protein Nitrogen CompoundspixiedustPas encore d'évaluation
- L-Ornithine L-Aspartate For The Treatment of SarcopeniaDocument7 pagesL-Ornithine L-Aspartate For The Treatment of SarcopeniaNabeel Ahmed KhanPas encore d'évaluation
- Consenso Saha 2Document12 pagesConsenso Saha 2RobertoPas encore d'évaluation
- FrancesFranciscoCC2 1Document6 pagesFrancesFranciscoCC2 1Frances FranciscoPas encore d'évaluation
- Aubf Lab PrelimsDocument14 pagesAubf Lab PrelimsFuture TrekingPas encore d'évaluation
- 17 Urinary SystemDocument5 pages17 Urinary SystemOribello, Athenna Jae W.Pas encore d'évaluation
- Presentation I PC II RENALDocument58 pagesPresentation I PC II RENALSuhayb CumarPas encore d'évaluation
- Maiuolo 2016Document7 pagesMaiuolo 2016okaPas encore d'évaluation
- Ratification Page: Andi Citra Pratiwi, S.PD, M.Ed Muhammad Nur Arsyad, S.PDDocument18 pagesRatification Page: Andi Citra Pratiwi, S.PD, M.Ed Muhammad Nur Arsyad, S.PDFatmawatiPas encore d'évaluation
- UricDocument9 pagesUricdr.yogaPas encore d'évaluation
- Intra Renal Cori CycleDocument21 pagesIntra Renal Cori Cyclesuman palPas encore d'évaluation
- Urea and Ammonia Metabolism and The Control of Renal Nitrogen ExcretionDocument15 pagesUrea and Ammonia Metabolism and The Control of Renal Nitrogen ExcretionJames Cojab SacalPas encore d'évaluation
- International Journal of Mathematics and Statistics Invention (IJMSI)Document8 pagesInternational Journal of Mathematics and Statistics Invention (IJMSI)inventionjournalsPas encore d'évaluation
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument20 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherraynanthaPas encore d'évaluation
- Dialysis Treatment - A Comprehensive DescriptionDocument13 pagesDialysis Treatment - A Comprehensive Descriptionrmprskgwk5Pas encore d'évaluation
- Support of Renal FunctionDocument9 pagesSupport of Renal FunctionImah ArmildezPas encore d'évaluation
- Uric Acid ProductionDocument21 pagesUric Acid ProductionNeha Srivastava0% (1)
- The Kidney, Excretion and OsmoregulationDocument63 pagesThe Kidney, Excretion and OsmoregulationJfoxx SamuelPas encore d'évaluation
- Anal. Clin. II Deter. UreaDocument15 pagesAnal. Clin. II Deter. UreaDilcerCernaPas encore d'évaluation
- Wella S, VIRINA Bsn-I: Review Question Urinary SystemDocument4 pagesWella S, VIRINA Bsn-I: Review Question Urinary SystemEllee HadesPas encore d'évaluation
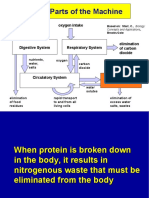
- Major Parts of The Machine: Food, Water Intake Oxygen IntakeDocument24 pagesMajor Parts of The Machine: Food, Water Intake Oxygen Intakecarl.lontoc2928Pas encore d'évaluation
- Uric Acid and Renal Function: Guilherme Ambrosio Albertoni, Fernanda Teixeira Borges and Nestor SchorDocument19 pagesUric Acid and Renal Function: Guilherme Ambrosio Albertoni, Fernanda Teixeira Borges and Nestor SchorYosuairvanPas encore d'évaluation
- QuestionsDocument4 pagesQuestionsA GoswamiPas encore d'évaluation
- Lab 4 5 Renal Functions TestDocument6 pagesLab 4 5 Renal Functions TestMustafa MahdiPas encore d'évaluation
- Watford 2003Document9 pagesWatford 2003josetuiran992Pas encore d'évaluation
- Renal System Anaphy LecDocument4 pagesRenal System Anaphy Lecbuenaveturajoshua95Pas encore d'évaluation
- VET343 Urinary Lecture Notes 2014Document35 pagesVET343 Urinary Lecture Notes 2014walczakcPas encore d'évaluation
- Urea Cycle4Document7 pagesUrea Cycle4Akinrotimi OluwadunsinPas encore d'évaluation
- Halymatu's ProjectDocument16 pagesHalymatu's ProjectNazifi AdamPas encore d'évaluation
- Edexcel Ial Biology Unit 5: The KidneyDocument24 pagesEdexcel Ial Biology Unit 5: The KidneyMithun ParanitharanPas encore d'évaluation
- Primary Care Approach To ProteinuriaDocument6 pagesPrimary Care Approach To Proteinuriadanny17phPas encore d'évaluation
- Kidney Function TestsDocument15 pagesKidney Function Testspntmai.y2020Pas encore d'évaluation
- Acute Renal FailureDocument30 pagesAcute Renal FailureRudra DasPas encore d'évaluation
- Human Physiology Ii: School of BiochemistryDocument15 pagesHuman Physiology Ii: School of Biochemistrykeerthana t reddyPas encore d'évaluation
- Urinary System 25 Feb 2013Document44 pagesUrinary System 25 Feb 2013adystiPas encore d'évaluation
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case StudyPrincess Tindugan100% (1)
- Primary Care Approach To Proteinuria: Amir Said Alizadeh Naderi, MD, and Robert F. Reilly, MDDocument6 pagesPrimary Care Approach To Proteinuria: Amir Said Alizadeh Naderi, MD, and Robert F. Reilly, MDDarian AngPas encore d'évaluation
- Analysis of Urine and Other Body Fluids: Introduction To Urinalysis Topic OutlineDocument6 pagesAnalysis of Urine and Other Body Fluids: Introduction To Urinalysis Topic OutlineBEVERLY JANE LLUVERASPas encore d'évaluation
- 4acid Base Balance and Renal Function TestsDocument50 pages4acid Base Balance and Renal Function TestsOsama MohamedPas encore d'évaluation
- 4 Excretory SystemDocument15 pages4 Excretory SystemBhavin ChangelaPas encore d'évaluation
- Berne y Levy 581-590Document10 pagesBerne y Levy 581-590Luis Miguel De LeonPas encore d'évaluation
- L-16 Purine Biochemistry and Uric Acid Metabolism - XMLDocument18 pagesL-16 Purine Biochemistry and Uric Acid Metabolism - XMLJulia HangaPas encore d'évaluation
- Course: Course Title: Course Credits: Contact Hours/week: Course DescriptionDocument24 pagesCourse: Course Title: Course Credits: Contact Hours/week: Course DescriptionNathaniel PulidoPas encore d'évaluation
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledD'EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledPas encore d'évaluation
- Kentucky Economic Development Guide 2010Document130 pagesKentucky Economic Development Guide 2010Journal CommunicationsPas encore d'évaluation
- Xiameter OFS-6020 Silane: Diaminofunctional Silane Features ApplicationsDocument2 pagesXiameter OFS-6020 Silane: Diaminofunctional Silane Features ApplicationsDelovita GintingPas encore d'évaluation
- Number SystemsDocument25 pagesNumber SystemsMehwish BilalPas encore d'évaluation
- Sullair VARIABLE SPEED - 1800-2200-1800V-1809V-2200V-25-30HPDocument70 pagesSullair VARIABLE SPEED - 1800-2200-1800V-1809V-2200V-25-30HPJose MontielPas encore d'évaluation
- Metric Conversion WorksheetDocument3 pagesMetric Conversion WorksheetKaiden HughesPas encore d'évaluation
- Installation Manual of FirmwareDocument6 pagesInstallation Manual of FirmwareOmar Stalin Lucio RonPas encore d'évaluation
- DEH-X500BT DEH-S4150BT: CD Rds Receiver Receptor de CD Con Rds CD Player Com RdsDocument53 pagesDEH-X500BT DEH-S4150BT: CD Rds Receiver Receptor de CD Con Rds CD Player Com RdsLUIS MANUEL RINCON100% (1)
- Doyennés Et Granges de L'abbaye de Cluny (A. Guerreau)Document45 pagesDoyennés Et Granges de L'abbaye de Cluny (A. Guerreau)theseus11Pas encore d'évaluation
- High Performance ComputingDocument294 pagesHigh Performance Computingsorinbazavan100% (1)
- Breaking News EnglishDocument13 pagesBreaking News English32. Nguyễn OanhPas encore d'évaluation
- RULE 130 Rules of CourtDocument141 pagesRULE 130 Rules of CourtalotcepilloPas encore d'évaluation
- How Do I Predict Event Timing Saturn Nakshatra PDFDocument5 pagesHow Do I Predict Event Timing Saturn Nakshatra PDFpiyushPas encore d'évaluation
- 1 Kane Equations - Example 1Document8 pages1 Kane Equations - Example 1Khisbullah HudhaPas encore d'évaluation
- MCQ With AnsDocument8 pagesMCQ With AnsAman KumarPas encore d'évaluation
- Format Mini Lesson Plan: What Is Narrative Text?Document3 pagesFormat Mini Lesson Plan: What Is Narrative Text?Muhammad FahrurajiPas encore d'évaluation
- Competency #14 Ay 2022-2023 Social StudiesDocument22 pagesCompetency #14 Ay 2022-2023 Social StudiesCharis RebanalPas encore d'évaluation
- Effect of Social Economic Factors On Profitability of Soya Bean in RwandaDocument7 pagesEffect of Social Economic Factors On Profitability of Soya Bean in RwandaMarjery Fiona ReyesPas encore d'évaluation
- 5 Waves AnswersDocument2 pages5 Waves AnswersNoor Ulain NabeelaPas encore d'évaluation
- Cottrell Park Golf Club 710Document11 pagesCottrell Park Golf Club 710Mulligan PlusPas encore d'évaluation
- Progress Test-The 7-Th GradeDocument2 pagesProgress Test-The 7-Th GradebabystelutaPas encore d'évaluation
- Simon Bolivar PresentationDocument7 pagesSimon Bolivar Presentationapi-345742212Pas encore d'évaluation
- 实用多元统计分析Document611 pages实用多元统计分析foo-hoat LimPas encore d'évaluation
- 8 - Packed Tower Design-1Document65 pages8 - Packed Tower Design-1M.H vafaeiPas encore d'évaluation
- Pset 2Document13 pagesPset 2rishiko aquinoPas encore d'évaluation