Vous aimerez peut-être aussi
- ITF Warlike and High Risk AreasDocument11 pagesITF Warlike and High Risk AreasDenis HranjPas encore d'évaluation
- 10.1007 - s12029 010 9200 XDocument8 pages10.1007 - s12029 010 9200 XDenis HranjPas encore d'évaluation
- ITF Warlike and High Risk AreasDocument11 pagesITF Warlike and High Risk AreasDenis HranjPas encore d'évaluation
- An ITF Guide For Seafarers To The ILO Maritime Labour Convention, 2006Document81 pagesAn ITF Guide For Seafarers To The ILO Maritime Labour Convention, 2006Mark Lourence TiuPas encore d'évaluation
- OJS File PDFDocument11 pagesOJS File PDFDenis HranjPas encore d'évaluation
- Issue 22 AccidentsDocument12 pagesIssue 22 AccidentsDenis HranjPas encore d'évaluation
- Ibf List: of Designated Risk Areas, With Applicable Benefits (As of 1 March 2018)Document11 pagesIbf List: of Designated Risk Areas, With Applicable Benefits (As of 1 March 2018)eds garciaPas encore d'évaluation
- Acton, Karen - Vespasian and The Social World of The Roman CourtDocument23 pagesActon, Karen - Vespasian and The Social World of The Roman CourtDenis HranjPas encore d'évaluation
- Morske Luke - 2006 2010Document167 pagesMorske Luke - 2006 2010Ivana RepalustPas encore d'évaluation
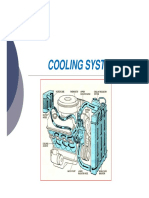
- Cooling SystemDocument45 pagesCooling SystemDenis HranjPas encore d'évaluation
- Roger Portal, "The Slavs", London 1969Document263 pagesRoger Portal, "The Slavs", London 1969Vasko Gligorijevic100% (4)
- 3512C and 3516C Marine Auxiliary Engines-Engine SafetyDocument12 pages3512C and 3516C Marine Auxiliary Engines-Engine SafetyDenis HranjPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Alcohol by DR Rizwan Zafar CMH Lahore Medical CollegeDocument58 pagesAlcohol by DR Rizwan Zafar CMH Lahore Medical CollegeRizwan Zafar AnsariPas encore d'évaluation
- Special Education ProcessDocument32 pagesSpecial Education ProcessJohn Kevin LumayagPas encore d'évaluation
- 5 7 07 Dr. Douglas Tucker, MD Report For CBX With Envelope For 5 11 07 Another OcrDocument5 pages5 7 07 Dr. Douglas Tucker, MD Report For CBX With Envelope For 5 11 07 Another OcrDoTheMacaRenoPas encore d'évaluation
- Anti Thyroid DrugsDocument22 pagesAnti Thyroid DrugsShahid HameedPas encore d'évaluation
- Chapter 3 Rationality of DrugsDocument56 pagesChapter 3 Rationality of DrugsS.Srinivasan ('Chinu'); Renu KhannaPas encore d'évaluation
- Drug Cards CNSDocument23 pagesDrug Cards CNSChristine Schroeder100% (2)
- Review - Presby Residency ManualDocument400 pagesReview - Presby Residency ManualSneha SutharPas encore d'évaluation
- Query ReplyDocument5 pagesQuery ReplyParakhModyPas encore d'évaluation
- Final Draft - Project 3Document8 pagesFinal Draft - Project 3api-710214550Pas encore d'évaluation
- Con TovaDocument2 pagesCon Tovasheik muhtasimPas encore d'évaluation
- Defn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andDocument5 pagesDefn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andSambit BeheraPas encore d'évaluation
- The Clinical Effectiveness and Costeffectiveness of Bariatric (Weight Loss) Surgery For Obesity: A Systematic Review and Economic EvaluationDocument230 pagesThe Clinical Effectiveness and Costeffectiveness of Bariatric (Weight Loss) Surgery For Obesity: A Systematic Review and Economic EvaluationhendersonPas encore d'évaluation
- Biotech BrochureDocument2 pagesBiotech BrochureBangtan ArmyPas encore d'évaluation
- 9 Months Marathon Training Plan - OdtDocument6 pages9 Months Marathon Training Plan - OdtMichaelKahnertPas encore d'évaluation
- Fluid and Electrolyte BalanceDocument83 pagesFluid and Electrolyte BalanceRubinaPas encore d'évaluation
- Nasogastric & Gavage - NsoDocument5 pagesNasogastric & Gavage - NsojamesPas encore d'évaluation
- Z50 Transducer Ficha Tecnica SheetDocument3 pagesZ50 Transducer Ficha Tecnica SheetMarcos CharmeloPas encore d'évaluation
- Trazissin® VASOPRESSIN INJECTION USP 20IU Per 1ml Solution For Injection Package Leaflet - Taj PharmaDocument1 pageTrazissin® VASOPRESSIN INJECTION USP 20IU Per 1ml Solution For Injection Package Leaflet - Taj PharmaTAJ PHARMA — A Health Care ProviderPas encore d'évaluation
- NRes1 AssignmentDocument2 pagesNRes1 AssignmentAinee MeuvinPas encore d'évaluation
- OperativenotesinsurgeryDocument9 pagesOperativenotesinsurgerySakib EhsanPas encore d'évaluation
- Penatalaksanaan Fisioterapi Pada Penderita Gangguan Nyeri Akibat Sindrom Piriformis Dengan Teknik Strain Counterstrain Dan Contract Relax StretchingDocument7 pagesPenatalaksanaan Fisioterapi Pada Penderita Gangguan Nyeri Akibat Sindrom Piriformis Dengan Teknik Strain Counterstrain Dan Contract Relax Stretchingchyntia eryonzaPas encore d'évaluation
- EM Boot Camp Course ManualDocument531 pagesEM Boot Camp Course ManualshortysdavidPas encore d'évaluation
- Best definition stem cell quiz questionsDocument6 pagesBest definition stem cell quiz questionsChoe Yoek Soek0% (1)
- MS Set 1Document6 pagesMS Set 1Julienne ManabatPas encore d'évaluation
- Fever: Clinical DescriptionDocument6 pagesFever: Clinical DescriptionNama ManaPas encore d'évaluation
- A CASE STUDY ON Chronic Renal FailureDocument2 pagesA CASE STUDY ON Chronic Renal FailureJake Yvan DizonPas encore d'évaluation
- Factors Affecting Inter Individual Variations in Drug ResponseDocument10 pagesFactors Affecting Inter Individual Variations in Drug Responsehumera50% (4)
- Organophosphorus Insecticide Induced Hemorrhagic Pancreatitis - A Case ReportDocument3 pagesOrganophosphorus Insecticide Induced Hemorrhagic Pancreatitis - A Case ReportIOSRjournalPas encore d'évaluation
- SOFA ScoreDocument9 pagesSOFA ScoreIfone takahepisPas encore d'évaluation
- 1st History PEdiaDocument6 pages1st History PEdiaDeepak BamPas encore d'évaluation