Vous aimerez peut-être aussi
- TB Workplace Policy & ProgramDocument3 pagesTB Workplace Policy & Programraighnejames19100% (2)
- Memorandum TO: Cbti Employee, Security Guards, Contractor/Subcontractor From: Cbti-Hsse Date: JUNE 19, 2020 RE: Personal Protective EquipmentDocument1 pageMemorandum TO: Cbti Employee, Security Guards, Contractor/Subcontractor From: Cbti-Hsse Date: JUNE 19, 2020 RE: Personal Protective EquipmentJerick Villones100% (2)
- Annual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)Document7 pagesAnnual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)Angelica Ponce100% (2)
- SAMPLE Filled Up - DOLE Employer's Work Accident ReportDocument1 pageSAMPLE Filled Up - DOLE Employer's Work Accident ReportМарк Артём Лимот Апалла78% (18)
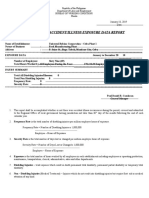
- Annual Work Accident/Illness Exposure Data Report: Dole/Bwc/Ohsd/Ip-6BDocument1 pageAnnual Work Accident/Illness Exposure Data Report: Dole/Bwc/Ohsd/Ip-6BMark Buendia91% (11)
- Annual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)Document7 pagesAnnual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)jaysonmalaa100% (2)
- Mental Health and Healthy Lifestyle Workplace Policy and ProgramDocument7 pagesMental Health and Healthy Lifestyle Workplace Policy and ProgramDarryl Robles100% (3)
- DOLE - FORM - WAIR - 1 - FOR - February 2023 PDFDocument1 pageDOLE - FORM - WAIR - 1 - FOR - February 2023 PDFKaren Jen100% (3)
- Instructions On How To Properly Fill in The WAIRDocument17 pagesInstructions On How To Properly Fill in The WAIRLauro CanceranPas encore d'évaluation
- OSH Program SampleDocument9 pagesOSH Program SampleLeah Ann AquinoPas encore d'évaluation
- Hepatitis B Workplace Policy & ProgramDocument4 pagesHepatitis B Workplace Policy & ProgramDiyames Ramos100% (3)
- Report On Health and Safety Organization Form (DOLE - BWC - OHSD - IP-5)Document2 pagesReport On Health and Safety Organization Form (DOLE - BWC - OHSD - IP-5)Randy Pedroza100% (6)
- Sample Report For Annual Health SafetyDocument2 pagesSample Report For Annual Health SafetyDian AvilaPas encore d'évaluation
- AEDR Annual Work Accident-Illness Exposure Data ReportDocument4 pagesAEDR Annual Work Accident-Illness Exposure Data ReportAlmario Sagun100% (1)
- Report of Safety and Health Organization MarilaoDocument1 pageReport of Safety and Health Organization MarilaoМарк Артём Лимот АпаллаPas encore d'évaluation
- Dole OSH ProgramDocument10 pagesDole OSH Programpolar1030090% (1)
- Annual Medical ReportDocument6 pagesAnnual Medical ReportMark BuendiaPas encore d'évaluation
- Osh Committee 2017Document3 pagesOsh Committee 2017jmmos207064100% (2)
- Rso DoleDocument1 pageRso DoleRERREFAIT100% (1)
- HIV AIDS Workplace - Policy and Program TemplateDocument4 pagesHIV AIDS Workplace - Policy and Program TemplatedebaynPas encore d'évaluation
- OSH Program-New FormatDocument14 pagesOSH Program-New FormatJesson PulmanoPas encore d'évaluation
- OSH Program Template (RA 11058)Document11 pagesOSH Program Template (RA 11058)Rodeth MarquezPas encore d'évaluation
- Breastfeeding Policy: Main Office Clark CDO Cebu Ilo-Ilo Davao Palawan WebsiteDocument2 pagesBreastfeeding Policy: Main Office Clark CDO Cebu Ilo-Ilo Davao Palawan Websitemark_ortencio100% (2)
- Hiv-Aids Workplace Policy and ProgramDocument4 pagesHiv-Aids Workplace Policy and ProgramluckyPas encore d'évaluation
- Hirac - DoleDocument11 pagesHirac - DoleAngela Salumbides50% (2)
- Dole Safety CommitteeDocument4 pagesDole Safety CommitteeМарк Артём Лимот АпаллаPas encore d'évaluation
- DOLE OSH Program TemplateDocument13 pagesDOLE OSH Program Templateoshc caraga100% (1)
- HMO Dependents Enrolment Form and Salary Deduction Authorization Form 20...Document1 pageHMO Dependents Enrolment Form and Salary Deduction Authorization Form 20...GemarieRoblesDelosReyesPas encore d'évaluation
- 5 - Drug-Free Workplace Policy and ProgramDocument5 pages5 - Drug-Free Workplace Policy and Programtangina moPas encore d'évaluation
- AEDR Annual Work Accident-Illness Exposure Data ReportDocument4 pagesAEDR Annual Work Accident-Illness Exposure Data ReportAlmario Sagun100% (1)
- 2021-11 Annex B Declaration and Undertaking - Res - 0Document1 page2021-11 Annex B Declaration and Undertaking - Res - 0Themie Lyn FaePas encore d'évaluation
- Wair Ip-6 PDFDocument2 pagesWair Ip-6 PDFJMPas encore d'évaluation
- Employer's Work Accident ReportDocument1 pageEmployer's Work Accident ReportAlex Elle0% (1)
- Employer's Work Accident - Illness Report Form (DOLE - BWC - OHSD - IP-6) DocDocument1 pageEmployer's Work Accident - Illness Report Form (DOLE - BWC - OHSD - IP-6) DocTsin Pajaro- Inocian100% (3)
- Dole BQF WairDocument5 pagesDole BQF Wairbeng acosta100% (1)
- Government Safety Engineer'S Accident Investigation ReportDocument1 pageGovernment Safety Engineer'S Accident Investigation ReportDon Aries EidosPas encore d'évaluation
- Wair ADocument2 pagesWair AJan Lenon Guira0% (1)
- RSO-Report On Health and Safety OrganizationDocument2 pagesRSO-Report On Health and Safety OrganizationAlaine Sobredo0% (1)
- Annual Work Accident Illness Exposure Data Report PDFDocument1 pageAnnual Work Accident Illness Exposure Data Report PDFedz100% (1)
- Report of Safety and Health OrganizationDocument1 pageReport of Safety and Health OrganizationМарк Артём Лимот АпаллаPas encore d'évaluation
- Annual Work Accident/Illness Exposure Data Report: General ManagerDocument1 pageAnnual Work Accident/Illness Exposure Data Report: General ManagerJamil DiligPas encore d'évaluation
- MINUTES OF MEETING AprilDocument2 pagesMINUTES OF MEETING AprilAlvin John DionisioPas encore d'évaluation
- Synerquest Breastfeeding PolicyDocument2 pagesSynerquest Breastfeeding PolicyRobin RubinaPas encore d'évaluation
- Fire Brigade Organizational ChartDocument1 pageFire Brigade Organizational ChartМарк Артём Лимот Апалла100% (2)
- Labor Advisory No. 08-23 Safety and Health Measures To Prevent and Control Heat Stress at The WorkplaceDocument2 pagesLabor Advisory No. 08-23 Safety and Health Measures To Prevent and Control Heat Stress at The WorkplaceRaymond Cruzin100% (1)
- Annual Medical Report FormDocument8 pagesAnnual Medical Report FormMarilou Mamaradlo100% (3)
- Safety - DOLE - Annual - Work - Accident - Incident - Exposure - Data Report (AWAIR)Document1 pageSafety - DOLE - Annual - Work - Accident - Incident - Exposure - Data Report (AWAIR)Dianna Baldoz-MijaresPas encore d'évaluation
- DOLE BWC OHSD IP 6bDocument1 pageDOLE BWC OHSD IP 6bYurs100% (1)
- Alcohol-Free Workplace Policy & ProgramDocument4 pagesAlcohol-Free Workplace Policy & Programraighnejames1950% (2)
- Dole BWC Ohsd Ip 5 Page 1Document2 pagesDole BWC Ohsd Ip 5 Page 1Yurs100% (1)
- Rso Ip5 PDFDocument1 pageRso Ip5 PDFJMPas encore d'évaluation
- Osh Program TemplateDocument12 pagesOsh Program TemplateMc alvinth SacletPas encore d'évaluation
- Sample TB Workplace Policy & ProgramDocument3 pagesSample TB Workplace Policy & ProgramJaniene SecuyaPas encore d'évaluation
- Aedr PDFDocument1 pageAedr PDFwindell PatalinghugPas encore d'évaluation
- Safety Practitioner Accreditation ChecklistDocument2 pagesSafety Practitioner Accreditation Checklistrasales100% (4)
- Employer'S Work Accident / Illness ReportDocument2 pagesEmployer'S Work Accident / Illness ReportDon Aries EidosPas encore d'évaluation
- Accident Report FormDocument2 pagesAccident Report Formengineermoelci1Pas encore d'évaluation
- Employer'S Work Accident / Illness ReportDocument2 pagesEmployer'S Work Accident / Illness ReportDon Aries EidosPas encore d'évaluation
- Republic of The Philippines Department of Labor and Employment Bureau of Working Conditions Manila Employer'S Work/Accident Illness ReportDocument2 pagesRepublic of The Philippines Department of Labor and Employment Bureau of Working Conditions Manila Employer'S Work/Accident Illness ReportEquilibrium EngineersPas encore d'évaluation
- LaborAdvisory No 07 22 WAIRDocument6 pagesLaborAdvisory No 07 22 WAIRRosalie LorenzoPas encore d'évaluation
- Wair FormatDocument1 pageWair FormatMc alvinth SacletPas encore d'évaluation
- WAIRDocument1 pageWAIRPrestonePas encore d'évaluation
- AmrDocument5 pagesAmrGemarie Adarlo CastilloPas encore d'évaluation
- Power Center CoverpageDocument1 pagePower Center CoverpageAlmario SagunPas encore d'évaluation
- Approved For Construction: Etron Bataan RefineryDocument1 pageApproved For Construction: Etron Bataan RefineryAlmario SagunPas encore d'évaluation
- Right Side Elevation C: A B C A B C B A CDocument1 pageRight Side Elevation C: A B C A B C B A CAlmario SagunPas encore d'évaluation
- Power Center - Structural RFA StructuralDocument1 pagePower Center - Structural RFA StructuralAlmario SagunPas encore d'évaluation
- Power Center Roof PlanDocument1 pagePower Center Roof PlanAlmario SagunPas encore d'évaluation
- Hilti HIT Rebar Design MethodDocument2 pagesHilti HIT Rebar Design MethodAlmario SagunPas encore d'évaluation
- Minutes of Pre-Bid Meeting & Scope of WorkDocument7 pagesMinutes of Pre-Bid Meeting & Scope of WorkAlmario Sagun100% (1)
- CEAM Technical Services Corp.: Petron Bataan RefineryDocument2 pagesCEAM Technical Services Corp.: Petron Bataan RefineryAlmario SagunPas encore d'évaluation
- M4 Bid Limestone Site DevtDocument12 pagesM4 Bid Limestone Site DevtAlmario SagunPas encore d'évaluation
- Warehouse Procedure of Project ConsumablesDocument28 pagesWarehouse Procedure of Project ConsumablesAlmario Sagun100% (4)
- Romeo EssayDocument3 pagesRomeo Essayapi-656725758Pas encore d'évaluation
- Section 19 of HMA ActDocument2 pagesSection 19 of HMA ActNandini SaikiaPas encore d'évaluation
- The Dog - Otto WeiningerDocument4 pagesThe Dog - Otto WeiningerstojanjovanovicPas encore d'évaluation
- Azari Mohd Rashid - Consultancy AgreementDocument6 pagesAzari Mohd Rashid - Consultancy AgreementRaymondPas encore d'évaluation
- Sales Final ReviewerDocument4 pagesSales Final ReviewerPhilipBrentMorales-MartirezCariagaPas encore d'évaluation
- SAGA v2 - Getting Started With The MongolsDocument4 pagesSAGA v2 - Getting Started With The Mongolsbaneblade1Pas encore d'évaluation
- United States Court of Appeals For The Third CircuitDocument22 pagesUnited States Court of Appeals For The Third CircuitScribd Government DocsPas encore d'évaluation
- Constitution: Article 3, Section 2Document4 pagesConstitution: Article 3, Section 2Marcos BallesterosPas encore d'évaluation
- The Shock of The New India-US RelationsDocument20 pagesThe Shock of The New India-US RelationspiyushPas encore d'évaluation
- Milk Code: Its Salient PointsDocument3 pagesMilk Code: Its Salient PointsLeah Abdul KabibPas encore d'évaluation
- TLD MilitaryDocument24 pagesTLD MilitarygmailPas encore d'évaluation
- Milton William CooperDocument97 pagesMilton William CoopertaurowillPas encore d'évaluation
- John Petsche IndictmentDocument2 pagesJohn Petsche IndictmentWKYC.comPas encore d'évaluation
- Transpo Case ReportDocument10 pagesTranspo Case ReportJesse AlindoganPas encore d'évaluation
- Arigo V SwiftDocument21 pagesArigo V SwiftKristine KristineeePas encore d'évaluation
- COMMISSION ON AUDIT CIRCULAR NO. 81-155 February 23, 1981Document7 pagesCOMMISSION ON AUDIT CIRCULAR NO. 81-155 February 23, 1981debate ddPas encore d'évaluation
- Romans Bible Study 32: Christian Liberty 2 - Romans 14:14-23Document4 pagesRomans Bible Study 32: Christian Liberty 2 - Romans 14:14-23Kevin MatthewsPas encore d'évaluation
- Significance of Black History MonthDocument6 pagesSignificance of Black History MonthRedemptah Mutheu MutuaPas encore d'évaluation
- Anthony Kaferle, Joe Brandstetter, John Kristoff and Mike Kristoff v. Stephen Fredrick, John Kosor and C. & F. Coal Company. C. & F. Coal Company, 360 F.2d 536, 3rd Cir. (1966)Document5 pagesAnthony Kaferle, Joe Brandstetter, John Kristoff and Mike Kristoff v. Stephen Fredrick, John Kosor and C. & F. Coal Company. C. & F. Coal Company, 360 F.2d 536, 3rd Cir. (1966)Scribd Government DocsPas encore d'évaluation
- Ballymun, Is The Place To Live inDocument10 pagesBallymun, Is The Place To Live inRita CahillPas encore d'évaluation
- Subiecte 8Document4 pagesSubiecte 8Mario TescanPas encore d'évaluation
- Afghan PakDocument48 pagesAfghan PakHifza ButtPas encore d'évaluation
- Esther Bible StudyDocument43 pagesEsther Bible StudyEsther Renda ItaarPas encore d'évaluation
- Assigment of literacture-WPS OfficeDocument4 pagesAssigment of literacture-WPS OfficeAakib Arijit ShaikhPas encore d'évaluation
- Deeng140 - 23242 - 1 3Document3 pagesDeeng140 - 23242 - 1 3azzyeemPas encore d'évaluation
- CRPC Syllabus 2017 Batch (1908)Document8 pagesCRPC Syllabus 2017 Batch (1908)soumya100% (1)
- ARIADocument3 pagesARIAangeli camillePas encore d'évaluation
- United States v. Calvin Lee Everette, 4th Cir. (2013)Document3 pagesUnited States v. Calvin Lee Everette, 4th Cir. (2013)Scribd Government DocsPas encore d'évaluation
- 9B Working UndercoverDocument4 pages9B Working UndercoverJorge Khouri JAKPas encore d'évaluation