Vous aimerez peut-être aussi
- Innovation in The Biopharmaceutical Pipeline-Analysis Group FinalDocument38 pagesInnovation in The Biopharmaceutical Pipeline-Analysis Group FinalAbhishek TomarPas encore d'évaluation
- Target Validation in Drug DiscoveryD'EverandTarget Validation in Drug DiscoveryBrian W. MetcalfPas encore d'évaluation
- Perspective: New England Journal MedicineDocument4 pagesPerspective: New England Journal MedicineYRHLI7389Pas encore d'évaluation
- Antibiotics 13 00072 v222Document22 pagesAntibiotics 13 00072 v222drnguyenbvtkPas encore d'évaluation
- College of Pharmacy: Different Phases of Clinical Trials With Elements To Be EvaluatedDocument11 pagesCollege of Pharmacy: Different Phases of Clinical Trials With Elements To Be EvaluatedSai Mani KrishnaPas encore d'évaluation
- Transforming Translation Impact of Clinical and Translational ScienceDocument3 pagesTransforming Translation Impact of Clinical and Translational ScienceSamPas encore d'évaluation
- Decision Points in NCE Development PDFDocument43 pagesDecision Points in NCE Development PDFprashantPas encore d'évaluation
- Drug DiscoveryDocument397 pagesDrug DiscoveryJane Hanrahan100% (1)
- Week 2: Post-Marketing Regulation of Pharmaceutical Products LearningDocument4 pagesWeek 2: Post-Marketing Regulation of Pharmaceutical Products LearningNics PedrezuelaPas encore d'évaluation
- Clinical Development ChapterDocument20 pagesClinical Development ChapterPooja Ramit KapoorPas encore d'évaluation
- Guidelines Phase1 Clinical TrialsDocument64 pagesGuidelines Phase1 Clinical TrialsJinnatPas encore d'évaluation
- Fphar 11 00733Document14 pagesFphar 11 00733Panos ArvanitisPas encore d'évaluation
- Coleman 2021Document10 pagesColeman 2021Pratul TiwariPas encore d'évaluation
- Ch6 19rareDocument4 pagesCh6 19rareArmin BiparvaPas encore d'évaluation
- Estudio CattieDocument18 pagesEstudio CattieMaría Alesia FernándezPas encore d'évaluation
- Ad Hoc Data SourcesDocument11 pagesAd Hoc Data SourcesVINAY KUMARPas encore d'évaluation
- FDA Paving Way For Personalized Medicine 62 Pages - 20140523Document62 pagesFDA Paving Way For Personalized Medicine 62 Pages - 20140523Dylan BruneauPas encore d'évaluation
- Huang 2013Document12 pagesHuang 2013GusgaraPas encore d'évaluation
- 10 - Drug DevelopmentDocument5 pages10 - Drug DevelopmentLaura SaglietiPas encore d'évaluation
- I E CriteriaReportFINALDocument12 pagesI E CriteriaReportFINALNanditha MPas encore d'évaluation
- SSRN Id1507457Document5 pagesSSRN Id1507457cmc.singh.mPas encore d'évaluation
- Perspective: New England Journal MedicineDocument4 pagesPerspective: New England Journal MedicineGary MaoPas encore d'évaluation
- Medicines Promotion: Assessing The Nature, Extent and Impact of RegulationDocument38 pagesMedicines Promotion: Assessing The Nature, Extent and Impact of RegulationAsmitaPas encore d'évaluation
- Misha Regulatory AffairsDocument26 pagesMisha Regulatory AffairsGULSHAN MADHURPas encore d'évaluation
- New Uses For Old DrugsDocument2 pagesNew Uses For Old DrugsJack JordanPas encore d'évaluation
- Applying Pharmacogenomics in Drug Development: Call For Collaborative EffortsDocument5 pagesApplying Pharmacogenomics in Drug Development: Call For Collaborative EffortsVeronica BalanPas encore d'évaluation
- Drug Discovery and Development Lecture NotesDocument75 pagesDrug Discovery and Development Lecture NotesJameel BakhshPas encore d'évaluation
- New Drug Application Content and Review Process For Clinical Pharmacology and BiopharmaceuticsDocument16 pagesNew Drug Application Content and Review Process For Clinical Pharmacology and BiopharmaceuticsAnki0391Pas encore d'évaluation
- 508 Paving Way For Personalized Medicine 2013 - ReducedDocument62 pages508 Paving Way For Personalized Medicine 2013 - Reduced88AKKPas encore d'évaluation
- Prospect For Covid-19 Investigational Drugs The Timeline (Prospect For Covid-19 Therapeutics)Document5 pagesProspect For Covid-19 Investigational Drugs The Timeline (Prospect For Covid-19 Therapeutics)International Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- 5) PharmacoepidemiologyDocument51 pages5) PharmacoepidemiologyDr. Zirwa AsimPas encore d'évaluation
- Comparison of Three Criteria For Potentially Inappropriate Medications in Chinese Older AdultsDocument8 pagesComparison of Three Criteria For Potentially Inappropriate Medications in Chinese Older AdultsSundas EjazPas encore d'évaluation
- Estimating The Incremental Net Health Benefit of Requirements For Cardiovascular Risk Evaluation For Diabetes TherapiesDocument21 pagesEstimating The Incremental Net Health Benefit of Requirements For Cardiovascular Risk Evaluation For Diabetes TherapiesDelia SeptiliaPas encore d'évaluation
- A Retrospective Cohort Study of Diabetes Mellitus and Antipsychotic Treatment in The United StatesDocument7 pagesA Retrospective Cohort Study of Diabetes Mellitus and Antipsychotic Treatment in The United StatesDeegh MudhaPas encore d'évaluation
- 1 s2.0 S2352771420301622 Main PDFDocument7 pages1 s2.0 S2352771420301622 Main PDFVella SufaPas encore d'évaluation
- IBM Watson - How Cognitive Computing Can Be AppliedDocument14 pagesIBM Watson - How Cognitive Computing Can Be AppliedraulfernandocoradoPas encore d'évaluation
- Industry Corner: Perspectives and Controversies ONCOLOGY 2020Document4 pagesIndustry Corner: Perspectives and Controversies ONCOLOGY 2020Ramiro TupayachiPas encore d'évaluation
- Clinpharm TranslationDocument4 pagesClinpharm TranslationAzizan HakimPas encore d'évaluation
- Jingchun Sun, A Systematic Analysis of FDA-approvedDocument17 pagesJingchun Sun, A Systematic Analysis of FDA-approvedAlejandro TurnerPas encore d'évaluation
- Polypill, Indications and Use 2.1Document12 pagesPolypill, Indications and Use 2.1jordiPas encore d'évaluation
- 2023 AJTM Vol 7 Issue 1 Article 7Document9 pages2023 AJTM Vol 7 Issue 1 Article 7gzou2013Pas encore d'évaluation
- Current PharmacoGenomics AssignmentDocument4 pagesCurrent PharmacoGenomics AssignmentShaher Bano MirzaPas encore d'évaluation
- Bio Markers Its Novel ApplicationDocument7 pagesBio Markers Its Novel ApplicationPharmacognosy JournalPas encore d'évaluation
- Development of Drugs To Treat TB (Dr. Daniel Everitt)Document40 pagesDevelopment of Drugs To Treat TB (Dr. Daniel Everitt)National Press FoundationPas encore d'évaluation
- Perspectives: How Many Drug Targets Are There?Document4 pagesPerspectives: How Many Drug Targets Are There?Mudit MisraPas encore d'évaluation
- 10 3233@jpd-202128Document18 pages10 3233@jpd-202128Elena AmaralPas encore d'évaluation
- Engels - 2007 - Medicinal Cannabis in OncologyDocument7 pagesEngels - 2007 - Medicinal Cannabis in OncologyRic Bil100% (1)
- Medicametos OmsDocument28 pagesMedicametos OmsKARLA LUCIA GARCIA PEREZPas encore d'évaluation
- Clinical and Translational Medicine Integrative AnDocument4 pagesClinical and Translational Medicine Integrative AnAJNCPas encore d'évaluation
- Cancer Biomarkers: Can We Turn Recent Failures Into Success?Document6 pagesCancer Biomarkers: Can We Turn Recent Failures Into Success?Anderson AlvesPas encore d'évaluation
- Personalized Medicine in Germany By: Ankit GurjarDocument12 pagesPersonalized Medicine in Germany By: Ankit GurjarAnkit Tonger AnkyPas encore d'évaluation
- Pew - Antibiotic PipelineDocument5 pagesPew - Antibiotic Pipelinetanishtarun06Pas encore d'évaluation
- Final Project LevofloxacinDocument102 pagesFinal Project LevofloxacinJalwaz TihamiPas encore d'évaluation
- Challenges To Use of Health-Related Quality of Life For Food and Drug Administration Approval of Anticancer ProductsDocument4 pagesChallenges To Use of Health-Related Quality of Life For Food and Drug Administration Approval of Anticancer Productsbasara_merlin6837Pas encore d'évaluation
- BiosimilarsDocument13 pagesBiosimilarsAhmed Abd El Aziz100% (1)
- Fphar 11 572569Document12 pagesFphar 11 572569hainguyen.htalabPas encore d'évaluation
- ASHP Guidelines On Handling Hazardous Drugs: 132 Drug Distribution and Control: Preparation and Handling-GuidelinesDocument33 pagesASHP Guidelines On Handling Hazardous Drugs: 132 Drug Distribution and Control: Preparation and Handling-GuidelinesNida NabilaPas encore d'évaluation
- Lista 2011 PDFDocument17 pagesLista 2011 PDFMaureen BorgesPas encore d'évaluation
- Handbook For GCPDocument132 pagesHandbook For GCPanotherlevel88Pas encore d'évaluation
- Final Project: Tabasco 7-Spice Chili Recipe Case Study MKTG - 1030 - F16Document9 pagesFinal Project: Tabasco 7-Spice Chili Recipe Case Study MKTG - 1030 - F16Kumar SaurabhPas encore d'évaluation
- JJ Kavanagh DiscountsDocument1 pageJJ Kavanagh DiscountsKumar SaurabhPas encore d'évaluation
- Sciencedirect: Indoor Environment Quality (User Comfort, Health and Behaviour)Document6 pagesSciencedirect: Indoor Environment Quality (User Comfort, Health and Behaviour)Kumar SaurabhPas encore d'évaluation
- Technological Forecasting & Social ChangeDocument17 pagesTechnological Forecasting & Social ChangeKumar SaurabhPas encore d'évaluation
- (Philosophy and Medicine 94) Mark J. Cherry, Ana Smith Iltis (Auth.), Mark J. Cherry, Ana Smith Iltis (Eds.) - Pluralistic Casuistry_ Moral Arguments, Economic Realities, And Political Theory-SpringerDocument260 pages(Philosophy and Medicine 94) Mark J. Cherry, Ana Smith Iltis (Auth.), Mark J. Cherry, Ana Smith Iltis (Eds.) - Pluralistic Casuistry_ Moral Arguments, Economic Realities, And Political Theory-SpringerKumar SaurabhPas encore d'évaluation
- 1 s2.0 S2211883719300206 MainDocument2 pages1 s2.0 S2211883719300206 MainKumar SaurabhPas encore d'évaluation
- Critical Perspectives On Accounting: Pauline Gleadle, Stuart Parris, Alan Shipman, Roberto SimonettiDocument11 pagesCritical Perspectives On Accounting: Pauline Gleadle, Stuart Parris, Alan Shipman, Roberto SimonettiKumar SaurabhPas encore d'évaluation
- Business Visa ChecklistDocument1 pageBusiness Visa ChecklistKumar SaurabhPas encore d'évaluation
- Dublinbikes Station Map 2017Document1 pageDublinbikes Station Map 2017Kumar SaurabhPas encore d'évaluation
- Czako VeronikaDocument371 pagesCzako VeronikaKumar SaurabhPas encore d'évaluation
- P 201707121200202017EMNIllegalEmploymentStudy Online 04.07.17Document67 pagesP 201707121200202017EMNIllegalEmploymentStudy Online 04.07.17Kumar SaurabhPas encore d'évaluation
- Semmler Et Al-2010-International Journal of ClimatologyDocument10 pagesSemmler Et Al-2010-International Journal of ClimatologyKumar SaurabhPas encore d'évaluation
- Lean Manufacturing in MalaysiaDocument7 pagesLean Manufacturing in MalaysiaSherazi MujtabaPas encore d'évaluation
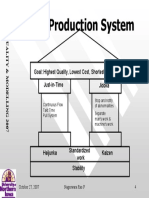
- Toyota Production SystemDocument1 pageToyota Production SystemKumar SaurabhPas encore d'évaluation
- FDR CallersDocument2 pagesFDR CallersKumar SaurabhPas encore d'évaluation
- National Diabetes Registry Report Vol 1 2009 2012 PDFDocument54 pagesNational Diabetes Registry Report Vol 1 2009 2012 PDFkhairul azlanPas encore d'évaluation
- KPMG Guide To SEZ in Poland 2009Document68 pagesKPMG Guide To SEZ in Poland 2009GNAFOOPas encore d'évaluation
- A Critical Study On Operations Managemen PDFDocument38 pagesA Critical Study On Operations Managemen PDFAAYUSH MALHOTRAPas encore d'évaluation
- Strategic Supply Chain Management The Development of A Diagnostic ModelDocument277 pagesStrategic Supply Chain Management The Development of A Diagnostic ModelKumar SaurabhPas encore d'évaluation
- Investment in Poland 2013Document150 pagesInvestment in Poland 2013Kumar SaurabhPas encore d'évaluation
- Technological Forecasting & Social ChangeDocument17 pagesTechnological Forecasting & Social ChangeKumar SaurabhPas encore d'évaluation
- What Is Social Capital?: by Yevoon 08533970 Otto 08532389Document22 pagesWhat Is Social Capital?: by Yevoon 08533970 Otto 08532389Kumar SaurabhPas encore d'évaluation
- Financial Management Formula TableDocument5 pagesFinancial Management Formula TableKumar SaurabhPas encore d'évaluation
- Ticket Vending Machines - PortugalDocument9 pagesTicket Vending Machines - Portugalan_outsiderPas encore d'évaluation
- Symposium S4Document8 pagesSymposium S4huykhiemPas encore d'évaluation
- IFPMA Facts and Figures 2017Document86 pagesIFPMA Facts and Figures 2017Destria Indah SariPas encore d'évaluation
- Critical Perspectives On Accounting: Pauline Gleadle, Stuart Parris, Alan Shipman, Roberto SimonettiDocument11 pagesCritical Perspectives On Accounting: Pauline Gleadle, Stuart Parris, Alan Shipman, Roberto SimonettiKumar SaurabhPas encore d'évaluation
- Gabbay 1999 Corporate Social Capital and LiabilityDocument559 pagesGabbay 1999 Corporate Social Capital and LiabilityKumar SaurabhPas encore d'évaluation
- Bourdieu 1986-The Forms of CapitalDocument19 pagesBourdieu 1986-The Forms of CapitalKumar SaurabhPas encore d'évaluation
- Hormones and The Menstrual Cycle: Discussion GuideDocument11 pagesHormones and The Menstrual Cycle: Discussion GuideJohnryl FranciscoPas encore d'évaluation
- All India Network Hospitals GeneralDocument630 pagesAll India Network Hospitals GeneralPankajPas encore d'évaluation
- PEH 11 Quarter 2 Module 5Document18 pagesPEH 11 Quarter 2 Module 5Aaliyah Kate100% (1)
- Clinical Effectiveness of Conservative ManagementDocument77 pagesClinical Effectiveness of Conservative ManagementD2S In'tl Business SolutionPas encore d'évaluation
- Discharge Plan 2.doc Imba - Doc123Document4 pagesDischarge Plan 2.doc Imba - Doc123Hezron Ga33% (3)
- MSDS Ultrachem Bond AcrDocument5 pagesMSDS Ultrachem Bond Acrjohan tindiPas encore d'évaluation
- 10 Physical and Mental Benefits of BasketballDocument4 pages10 Physical and Mental Benefits of BasketballJohn Kenzo NavatoPas encore d'évaluation
- 11 Strategies To Fight CancerDocument73 pages11 Strategies To Fight CancerPayal Nandwana100% (1)
- Why To Not Legalize EuthanasiaDocument5 pagesWhy To Not Legalize EuthanasiaScotiaccap2016Pas encore d'évaluation
- The 5x5 ProgramDocument13 pagesThe 5x5 ProgramSMO979Pas encore d'évaluation
- Medical Devices - Definition, Classification and RegulationDocument11 pagesMedical Devices - Definition, Classification and RegulationAaltiya100% (1)
- Structural Family Therapy Versus Strategic Family Therapy: A Comparative DiscussionDocument11 pagesStructural Family Therapy Versus Strategic Family Therapy: A Comparative DiscussionDavid P Sanchez100% (8)
- Activity Completion Report: District of Basey IDocument2 pagesActivity Completion Report: District of Basey IRyan Adona GaddiPas encore d'évaluation
- Romany Lofty: Prepare byDocument27 pagesRomany Lofty: Prepare bySupekshya ShresthaPas encore d'évaluation
- Making Every School A Health-Promoting School: Implementation GuidanceDocument89 pagesMaking Every School A Health-Promoting School: Implementation GuidancePablo MateusPas encore d'évaluation
- Standardized Curriculum in General Surgery 2012Document102 pagesStandardized Curriculum in General Surgery 2012Martin EscasuraPas encore d'évaluation
- The Complex PTSD Workbook: A Mind-Body Approach To Regaining Emotional Control and Becoming Whole - PathologiesDocument5 pagesThe Complex PTSD Workbook: A Mind-Body Approach To Regaining Emotional Control and Becoming Whole - Pathologiesnaruzebi10% (21)
- Theory ApplicationDocument8 pagesTheory Applicationaileen Dinglasan50% (2)
- Basic Principal of NaturopathyDocument3 pagesBasic Principal of Naturopathyniketlekariya100% (1)
- A Chamber of Secrets The Neurology of The Thalamus - Lessons From Acute StrokeDocument6 pagesA Chamber of Secrets The Neurology of The Thalamus - Lessons From Acute StrokeIvan Morales BarreraPas encore d'évaluation
- COG Chemo Admin GuidelinesDocument38 pagesCOG Chemo Admin GuidelinesCristina Georgiana ZahariaPas encore d'évaluation
- Personality DisordersDocument128 pagesPersonality DisordersKirsten100% (9)
- SLRC Pedia PresentationDocument141 pagesSLRC Pedia Presentationapi-3764215100% (2)
- Literature Review Network SecurityDocument8 pagesLiterature Review Network Securityc5q8g5tz100% (1)
- Intimacy in MarriageDocument9 pagesIntimacy in MarriageGaryPas encore d'évaluation
- Mind FitnessDocument9 pagesMind FitnessFit DealsPas encore d'évaluation
- Asfiksia JurnalDocument9 pagesAsfiksia JurnalGung Citra PratikaPas encore d'évaluation
- Regulatory Bodies of Nursing in India: Dr. Maheswari JaikumarDocument75 pagesRegulatory Bodies of Nursing in India: Dr. Maheswari Jaikumarkalla sharonPas encore d'évaluation
- Aaa Gastrectomy NCP FinalDocument13 pagesAaa Gastrectomy NCP Finallexzaf100% (1)
- Acetaminophen TylenolDocument2 pagesAcetaminophen TylenolKristi WrayPas encore d'évaluation
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildD'EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildÉvaluation : 3.5 sur 5 étoiles3.5/5 (9)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductD'EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductÉvaluation : 5 sur 5 étoiles5/5 (31)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryD'EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryÉvaluation : 5 sur 5 étoiles5/5 (47)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionD'EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryD'EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryPas encore d'évaluation
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.D'EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Évaluation : 4 sur 5 étoiles4/5 (7)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousD'EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousÉvaluation : 5 sur 5 étoiles5/5 (22)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsD'EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsPas encore d'évaluation
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsD'EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsÉvaluation : 4.5 sur 5 étoiles4.5/5 (6)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerD'EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerÉvaluation : 5 sur 5 étoiles5/5 (8)
- Little Red Book: Alcoholics AnonymousD'EverandLittle Red Book: Alcoholics AnonymousÉvaluation : 5 sur 5 étoiles5/5 (20)
- Food of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionD'EverandFood of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionÉvaluation : 4.5 sur 5 étoiles4.5/5 (117)
- Stop Drinking Now: The original Easyway methodD'EverandStop Drinking Now: The original Easyway methodÉvaluation : 5 sur 5 étoiles5/5 (28)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingD'EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingÉvaluation : 5 sur 5 étoiles5/5 (11)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionD'EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionÉvaluation : 5 sur 5 étoiles5/5 (63)
- Quitting Smoking & Vaping For Dummies: 2nd EditionD'EverandQuitting Smoking & Vaping For Dummies: 2nd EditionPas encore d'évaluation
- Blood Orange Night: My Journey to the Edge of MadnessD'EverandBlood Orange Night: My Journey to the Edge of MadnessÉvaluation : 4 sur 5 étoiles4/5 (42)
- You Are More Than This Will Ever Be: Methamphetamine: The Dirty DrugD'EverandYou Are More Than This Will Ever Be: Methamphetamine: The Dirty DrugPas encore d'évaluation
- Stop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenD'EverandStop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenÉvaluation : 5 sur 5 étoiles5/5 (62)
- Easyway Express: Stop Smoking and Quit E-CigarettesD'EverandEasyway Express: Stop Smoking and Quit E-CigarettesÉvaluation : 5 sur 5 étoiles5/5 (15)
- Healing the Scars of Addiction: Reclaiming Your Life and Moving into a Healthy FutureD'EverandHealing the Scars of Addiction: Reclaiming Your Life and Moving into a Healthy FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (7)
- Summary of Gary Wilson's Your Brain on PornD'EverandSummary of Gary Wilson's Your Brain on PornÉvaluation : 5 sur 5 étoiles5/5 (1)
- Recovery 2.0: Move Beyond Addiction and Upgrade Your LifeD'EverandRecovery 2.0: Move Beyond Addiction and Upgrade Your LifeÉvaluation : 5 sur 5 étoiles5/5 (8)
- Addictions: A Banquet in the Grave: Finding Hope in the Power of the GospelD'EverandAddictions: A Banquet in the Grave: Finding Hope in the Power of the GospelÉvaluation : 4.5 sur 5 étoiles4.5/5 (11)
- Alcoholics Anonymous: The Landmark of Recovery and Vital LivingD'EverandAlcoholics Anonymous: The Landmark of Recovery and Vital LivingÉvaluation : 4.5 sur 5 étoiles4.5/5 (291)