Vous aimerez peut-être aussi
- Case Studies in Not-for-Profit Accounting and AuditingD'EverandCase Studies in Not-for-Profit Accounting and AuditingPas encore d'évaluation
- A. B. Certified: Certified: Allotment Available and ObligatedDocument3 pagesA. B. Certified: Certified: Allotment Available and ObligatedMatias WinnerPas encore d'évaluation
- No.: - Date: - Agency FundDocument11 pagesNo.: - Date: - Agency Fundlegal.darposaranganiPas encore d'évaluation
- Obligation 2024Document1 pageObligation 2024Lovelyn SeverinoPas encore d'évaluation
- Travel OrderDocument4 pagesTravel OrderAldrin NolascoPas encore d'évaluation
- Appendix 11 ORSDocument4 pagesAppendix 11 ORSgennadacawePas encore d'évaluation
- No.: - Date: - Agency FundDocument12 pagesNo.: - Date: - Agency Fundlegal.darposaranganiPas encore d'évaluation
- Obligation Request and StatusDocument12 pagesObligation Request and Statusmichael ricafortPas encore d'évaluation
- Sir PioDocument8 pagesSir PioREGIONAL DIRECTOR SOUTHERN TAGALOG0% (1)
- Attachments For NLC 1 1Document34 pagesAttachments For NLC 1 1Jessica CrisostomoPas encore d'évaluation
- DV Appendix 32-DECEMBER 2019 JHSDocument7 pagesDV Appendix 32-DECEMBER 2019 JHSRomel BayabanPas encore d'évaluation
- Annex A Budget SlipDocument3 pagesAnnex A Budget SlipMark HernandezPas encore d'évaluation
- OBR Representation June 2019Document2 pagesOBR Representation June 2019Kim MonteronaPas encore d'évaluation
- Budget Utilization Request StatusDocument11 pagesBudget Utilization Request Statusjef repuldaPas encore d'évaluation
- Obligation Request and Status: Appendix 11Document45 pagesObligation Request and Status: Appendix 11Kevin Verdan CambaPas encore d'évaluation
- Disbursement Form DivisionDocument2 pagesDisbursement Form DivisionShovy VillegasPas encore d'évaluation
- ORS DV-d.o.Document2 pagesORS DV-d.o.Jessica CrisostomoPas encore d'évaluation
- ORS 2021 (AutoRecovered)Document23 pagesORS 2021 (AutoRecovered)Theresa Faye De GuzmanPas encore d'évaluation
- Budget Utilization Request and Status: Nenita L.MarcosDocument2 pagesBudget Utilization Request and Status: Nenita L.MarcosMemphis RainsPas encore d'évaluation
- Liam BolecheDocument5 pagesLiam BolechemayrubienythPas encore d'évaluation
- P.O. (Fuel) JAN 2017 MaribertDocument3 pagesP.O. (Fuel) JAN 2017 MaribertRuss TuazonPas encore d'évaluation
- ORS Appendix 11-DECEMBER 2019 JHSDocument3 pagesORS Appendix 11-DECEMBER 2019 JHSRomel BayabanPas encore d'évaluation
- SDO-PM/WIM-QF-OSDS-FS-ACC-001Document75 pagesSDO-PM/WIM-QF-OSDS-FS-ACC-001Shiela E. EladPas encore d'évaluation
- Pagadian DV Bur BirDocument4 pagesPagadian DV Bur BirJayBalaPas encore d'évaluation
- DARPO Lanao del Norte Obligation Request and Status ReportDocument4 pagesDARPO Lanao del Norte Obligation Request and Status ReportmikzhiPas encore d'évaluation
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesSheryl SitoyPas encore d'évaluation
- FURS-1Document1 pageFURS-1YHONG SILVANOPas encore d'évaluation
- 2 Obligation Request & StatusDocument2 pages2 Obligation Request & Statusjoan dalilisPas encore d'évaluation
- TESDA Payment for Services RenderedDocument48 pagesTESDA Payment for Services RenderedAmadeus BurgeoisPas encore d'évaluation
- BIIS Blank DV and 2307Document3 pagesBIIS Blank DV and 2307spayumo821Pas encore d'évaluation
- Liquidation FormDocument4 pagesLiquidation FormMarlyn E. Azurin100% (1)
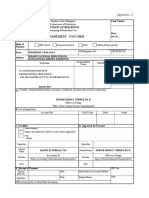
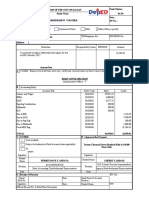
- Disbursement VoucherDocument5 pagesDisbursement VoucherFonzy RonePas encore d'évaluation
- 2022 Tev AprilDocument12 pages2022 Tev AprilJanus MariPas encore d'évaluation
- DISBURSEMENT Voucher SampleDocument16 pagesDISBURSEMENT Voucher SampleRachelle Rellora50% (2)
- Itinerary JOANDocument4 pagesItinerary JOANmin estigoyPas encore d'évaluation
- To Payment of Electricity Expenses For The Period of - As Per Billing Statement Hereto AttachedDocument6 pagesTo Payment of Electricity Expenses For The Period of - As Per Billing Statement Hereto AttachedShiela E. EladPas encore d'évaluation
- Obligation Request and Status: Appendix 11Document2 pagesObligation Request and Status: Appendix 11Cj NightsirkPas encore d'évaluation
- Obligation Request and Status: Dilg Car Entity Name Dilg Car Cos Personnel-Contact TracersDocument3 pagesObligation Request and Status: Dilg Car Entity Name Dilg Car Cos Personnel-Contact TracersClaudine PuyaoPas encore d'évaluation
- Different Forms (OBR, DV, Etc.) - As of 2017Document28 pagesDifferent Forms (OBR, DV, Etc.) - As of 2017DennisEstrellosoAlbisoPas encore d'évaluation
- Disbursement VoucherDocument1 pageDisbursement VoucherGeorgina Intia100% (1)
- RorfDocument2 pagesRorfGlenda Ducay ManotaPas encore d'évaluation
- Disbursement Voucher. Butuan BauleteDocument2 pagesDisbursement Voucher. Butuan BauleteTantan Oropa100% (1)
- DV Appendix 32-DECEMBER 2019 JHSDocument7 pagesDV Appendix 32-DECEMBER 2019 JHSRomel BayabanPas encore d'évaluation
- Year End Bonus PaymentDocument9 pagesYear End Bonus PaymentloretaPas encore d'évaluation
- T.O Voucher Ms NavalesDocument13 pagesT.O Voucher Ms Navalesarmand rodriguezPas encore d'évaluation
- Department of Education Fund Disbursement RecordsDocument7 pagesDepartment of Education Fund Disbursement RecordsLex AmariePas encore d'évaluation
- Fai1. DISBURSEMENT VOUCHER 3 COPIESDocument56 pagesFai1. DISBURSEMENT VOUCHER 3 COPIESagong lodgePas encore d'évaluation
- Mooe School Forms 2020Document40 pagesMooe School Forms 2020Bat RicPas encore d'évaluation
- Appendix 32 Fund Cluster DisbursementDocument2 pagesAppendix 32 Fund Cluster DisbursementSaripa Layatan MaruhomPas encore d'évaluation
- Carpentry Supplies 1Document12 pagesCarpentry Supplies 1Robinson ConcordiaPas encore d'évaluation
- Disbursement Voucher: Division of BukidnonDocument8 pagesDisbursement Voucher: Division of BukidnonJessica Prias MoscardonPas encore d'évaluation
- Supplemental-salary-DV, ORS, PAYROLLDocument4 pagesSupplemental-salary-DV, ORS, PAYROLLAllen Rey YeclaPas encore d'évaluation
- OBR For MOOE DownloadingDocument1 pageOBR For MOOE DownloadingAko Si KulitzPas encore d'évaluation
- Disbursement Voucher: Schools Division of AlbayDocument9 pagesDisbursement Voucher: Schools Division of AlbayJoseph NoblezaPas encore d'évaluation
- OBR-for-MOOE-downloadingDocument1 pageOBR-for-MOOE-downloadingJoan A. DagdagPas encore d'évaluation
- DV - July 2023 LindiDocument1 pageDV - July 2023 LindiAlbert Alonto DipatuanPas encore d'évaluation
- DISBURSEMENT VOUCHER (JC) - AugustDocument2 pagesDISBURSEMENT VOUCHER (JC) - Augusthekeho3180Pas encore d'évaluation
- COA Obligation and Disbursement RecordsDocument7 pagesCOA Obligation and Disbursement RecordsAddy GuinalPas encore d'évaluation
- DV ProposalDocument22 pagesDV ProposalMaria Avegail Balane EstradaPas encore d'évaluation
- IFLS Form & Surety 2023-24Document2 pagesIFLS Form & Surety 2023-24Muhammad SaeedPas encore d'évaluation
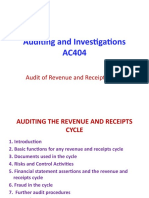
- AC404 - Revenue and Receipts Cycle Class NotesDocument38 pagesAC404 - Revenue and Receipts Cycle Class NotesObey KamutsamombePas encore d'évaluation
- A Comprehensive Report On The Rice Export BusinessDocument12 pagesA Comprehensive Report On The Rice Export BusinessMuhammad UmarPas encore d'évaluation
- SAP MM Config of Logistic Invoice Verification 1666406315Document15 pagesSAP MM Config of Logistic Invoice Verification 1666406315J S PRADEEP KUMARPas encore d'évaluation
- CH 3 Audit IIDocument21 pagesCH 3 Audit IIsamuel debebePas encore d'évaluation
- TAX-303 (Input Taxes)Document7 pagesTAX-303 (Input Taxes)Princess ManaloPas encore d'évaluation
- QS-F-8.1-4version 1.0Document2 pagesQS-F-8.1-4version 1.0Mohammad AkilPas encore d'évaluation
- SWBL Progress SheetDocument6 pagesSWBL Progress SheetNeil Ian Seth BacaniPas encore d'évaluation
- Suppliers Summary - 2020Document32 pagesSuppliers Summary - 2020Niera DelossantisPas encore d'évaluation
- Tax 301 - Vat-Subject TransactionsDocument10 pagesTax 301 - Vat-Subject TransactionsiBEAYPas encore d'évaluation
- CPRS StepDocument10 pagesCPRS StepJojie TayabanPas encore d'évaluation
- Resume Now RefundDocument8 pagesResume Now Refunduifujzhfg100% (2)
- Test-King.C - TB1200 - 90.70 QuestionsDocument30 pagesTest-King.C - TB1200 - 90.70 QuestionsNatnael KoraPas encore d'évaluation
- Charge Back BasicsDocument30 pagesCharge Back BasicsBui Xuan PhongPas encore d'évaluation
- Ncert Books PDF: Receipt and Payment Rules 1983 MCQDocument4 pagesNcert Books PDF: Receipt and Payment Rules 1983 MCQRISHABH TOMARPas encore d'évaluation
- RACI Matriks ATR Read OnlyDocument6 pagesRACI Matriks ATR Read OnlyAnup PandeyPas encore d'évaluation
- Tax Setup DocumentDocument26 pagesTax Setup DocumentManish BhansaliPas encore d'évaluation
- Configuring Invoice Approval Workflow-R12Document32 pagesConfiguring Invoice Approval Workflow-R12kriole130% (1)
- Project Release InterfacesDocument5 pagesProject Release InterfacesSritam MohantyPas encore d'évaluation
- Cpar Ngas & NpoDocument6 pagesCpar Ngas & NpoSittie Ainna A. UntePas encore d'évaluation
- Ocp Legazpi City 2019Document5 pagesOcp Legazpi City 2019Richard GuiribaPas encore d'évaluation
- Final Internship ReportDocument10 pagesFinal Internship ReportMaryam NisarPas encore d'évaluation
- Shipment Details: 3 1 0 4 7 3 1 1 6 2 Inbound ChargesDocument1 pageShipment Details: 3 1 0 4 7 3 1 1 6 2 Inbound ChargesChamaraPas encore d'évaluation
- Transaction keys guideDocument8 pagesTransaction keys guideKamleshSarojPas encore d'évaluation
- SMT Harleen Kaur Bhatiavs Principal Commissionerof IncomDocument23 pagesSMT Harleen Kaur Bhatiavs Principal Commissionerof IncomKaran GannaPas encore d'évaluation
- Intercompany Sales OrderDocument3 pagesIntercompany Sales OrderMark SanchezPas encore d'évaluation
- Receive and Process Reservation: Teaching and Learning MaterialsDocument31 pagesReceive and Process Reservation: Teaching and Learning MaterialsAdrita GusdilaPas encore d'évaluation
- Internal Order Accounting2Document39 pagesInternal Order Accounting2Ibbu MohdPas encore d'évaluation
- Fundamentals of Accountancy Books and JournalsDocument36 pagesFundamentals of Accountancy Books and JournalsLevi CorralPas encore d'évaluation
- Taganito Mining v. CIRDocument60 pagesTaganito Mining v. CIRaudreydql50% (1)
- Hostel Brochure Revised 2015-16 PDFDocument7 pagesHostel Brochure Revised 2015-16 PDFUday GulghanePas encore d'évaluation