Vous aimerez peut-être aussi
- Psychosis 0 PDFDocument4 pagesPsychosis 0 PDFGrace LPas encore d'évaluation
- Kymco Stryker 125 Parts CatalogueDocument138 pagesKymco Stryker 125 Parts CataloguejonnykPas encore d'évaluation
- Non-Addictive Painkillers: Recent Research and Development Braden Royer Dubois Area High School Honors Biochemistry Mr. KeithDocument11 pagesNon-Addictive Painkillers: Recent Research and Development Braden Royer Dubois Area High School Honors Biochemistry Mr. Keithapi-318355342Pas encore d'évaluation
- Opioid PharmacologyDocument47 pagesOpioid PharmacologyEva K. Al KaryPas encore d'évaluation
- Psychoactive DrugDocument21 pagesPsychoactive DrugRagnar Jose RaskockPas encore d'évaluation
- Executive Summary: Pain ManagementDocument116 pagesExecutive Summary: Pain ManagementErin MachnikPas encore d'évaluation
- Prescription Opioid Analgesics Rapidly Change The Human BrainDocument8 pagesPrescription Opioid Analgesics Rapidly Change The Human BrainboboPas encore d'évaluation
- Androgen ReceptorDocument5 pagesAndrogen ReceptorNandia SeptiyoriniPas encore d'évaluation
- Drugs of Abuse: Rita Dries Senior Lecturer KHK Turnhout - BelgiëDocument32 pagesDrugs of Abuse: Rita Dries Senior Lecturer KHK Turnhout - BelgiëKartikPas encore d'évaluation
- Analgesics: L. SchefflerDocument32 pagesAnalgesics: L. SchefflerNovita_PemalangPas encore d'évaluation
- DMT From M PDFDocument1 pageDMT From M PDFcaptaina1840Pas encore d'évaluation
- SedativeDocument35 pagesSedativeking_goldPas encore d'évaluation
- 1 Analgesics PDFDocument4 pages1 Analgesics PDFSimranPas encore d'évaluation
- Emerging Drugs of AbuseDocument4 pagesEmerging Drugs of AbuseKhaled KhapiPas encore d'évaluation
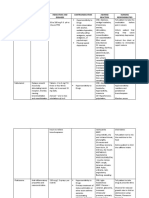
- Name of Drug Dosage/Route Mechanism of Action/ Classification Indication/Contraindication Side/Adverse Effects Nursing ConsiderationsDocument3 pagesName of Drug Dosage/Route Mechanism of Action/ Classification Indication/Contraindication Side/Adverse Effects Nursing ConsiderationsMonica Gagarin CortezPas encore d'évaluation
- Therapeutic Class: Anxiolytic Pharmacologic Class: Benzodiazepine Therapeutic Class: Anxiolytic Pharmacologic Class: BenzodiazepineDocument5 pagesTherapeutic Class: Anxiolytic Pharmacologic Class: Benzodiazepine Therapeutic Class: Anxiolytic Pharmacologic Class: BenzodiazepineAriadne MangondatoPas encore d'évaluation
- Psychoactive Drug UseDocument1 pagePsychoactive Drug UsePisay Shehannah Grail MedinaPas encore d'évaluation
- CNS StimulantDocument26 pagesCNS StimulantIslam Abdo50% (2)
- 4853 Medication Worksheet: Student NameDocument8 pages4853 Medication Worksheet: Student Nameapi-546817891Pas encore d'évaluation
- Effects of Emg Biofeedback On Pain and Quality of Life in Cervical Dystonia 2329 6895.1000144Document6 pagesEffects of Emg Biofeedback On Pain and Quality of Life in Cervical Dystonia 2329 6895.1000144danishmujibPas encore d'évaluation
- Case 5 - (Salimbagat) Drug StudyDocument4 pagesCase 5 - (Salimbagat) Drug StudyChristine Pialan SalimbagatPas encore d'évaluation
- Substance Abuse and Traumatic Brain Injury: John D. Corrigan, PHDDocument50 pagesSubstance Abuse and Traumatic Brain Injury: John D. Corrigan, PHDSilvanaPutriPas encore d'évaluation
- A02 269 PDFDocument97 pagesA02 269 PDFjaimePas encore d'évaluation
- Indication and DosagesDocument2 pagesIndication and DosagesloveskissesPas encore d'évaluation
- Principles of Fluid ChillersDocument7 pagesPrinciples of Fluid ChillersAzim AdamPas encore d'évaluation
- Xerophilia 2020 26 1Document14 pagesXerophilia 2020 26 1Nacho MartinezPas encore d'évaluation
- Drug Abuse and Drug Dependence: DR Keli F Med III LecturesDocument49 pagesDrug Abuse and Drug Dependence: DR Keli F Med III LecturestheintrovPas encore d'évaluation
- Drug Study GalaponDocument4 pagesDrug Study GalaponSheryl DiazPas encore d'évaluation
- Concise Manual of ElectricityDocument130 pagesConcise Manual of ElectricityBách HợpPas encore d'évaluation
- The Anti Reward Brain SystemDocument42 pagesThe Anti Reward Brain Systemtadcp100% (1)
- GHB PresentationDocument19 pagesGHB PresentationScorpion legionPas encore d'évaluation
- The Clinical Toxicology of Metamfetamine: ISSN: 1556-3650 Print / 1556-9519 Online DOI: 10.3109/15563650.2010.516752Document21 pagesThe Clinical Toxicology of Metamfetamine: ISSN: 1556-3650 Print / 1556-9519 Online DOI: 10.3109/15563650.2010.516752Miftahul Choir AlfarisiPas encore d'évaluation
- The BrainDocument7 pagesThe BrainCUESCANO, CRISTEL G. BSMT 2-APas encore d'évaluation
- n0 Alcohol Hangover, Business - PlanDocument20 pagesn0 Alcohol Hangover, Business - PlanVaguePas encore d'évaluation
- Samsung Galaxy A32 5G User Manual-EnglishDocument159 pagesSamsung Galaxy A32 5G User Manual-EnglishEgg Bread100% (1)
- Service Manual: Domestic Air ConditionerDocument20 pagesService Manual: Domestic Air Conditionerhernandez.josedomingo6804Pas encore d'évaluation
- 33+Rear+Axle,+Rear Wheel+Drive,+GuideDocument113 pages33+Rear+Axle,+Rear Wheel+Drive,+GuideRAUL RODRIGUEZ CERRO100% (1)
- Fentanyl - Duragesic (Analgesic, Narcotic, General Anesthetic)Document1 pageFentanyl - Duragesic (Analgesic, Narcotic, General Anesthetic)Danielle Marie SamblacenoPas encore d'évaluation
- 2019 Rec Drugs 1Document47 pages2019 Rec Drugs 1gowod86101Pas encore d'évaluation
- Amphetamines: Fatin Norhanani Binti Mohamad Najib Group 39Document9 pagesAmphetamines: Fatin Norhanani Binti Mohamad Najib Group 39FatinNorhananiPas encore d'évaluation
- MethDocument4 pagesMethapi-218061588Pas encore d'évaluation
- NIH Public Access: Active Emergence From Propofol General Anesthesia Is Induced by MethylphenidateDocument16 pagesNIH Public Access: Active Emergence From Propofol General Anesthesia Is Induced by Methylphenidate'-dooublleaiienn Itouehh IinPas encore d'évaluation
- 1 Jan 13 PDFDocument8 pages1 Jan 13 PDFAlejandroPas encore d'évaluation
- Drugs Interaction: DR - Datten Bangun MSC, SPFK & DR - Dr.Tri Widyawati MSCDocument39 pagesDrugs Interaction: DR - Datten Bangun MSC, SPFK & DR - Dr.Tri Widyawati MSCpsyPas encore d'évaluation
- Amphetamines: Short-Term EffectsDocument2 pagesAmphetamines: Short-Term EffectsAstari RidhanyaPas encore d'évaluation
- Lenovo ThinkPad HelixDocument6 pagesLenovo ThinkPad HelixkakarotoPas encore d'évaluation
- Drugs Acting On Adrenrgic Nervous System: Presented byDocument63 pagesDrugs Acting On Adrenrgic Nervous System: Presented byKiranPas encore d'évaluation
- Shimano Nexus3 178 ManualDocument12 pagesShimano Nexus3 178 Manualgrazka20Pas encore d'évaluation
- Mechanisms of Drug Interactions: Pharmacodynamics and PharmacokineticsDocument4 pagesMechanisms of Drug Interactions: Pharmacodynamics and Pharmacokineticsgowepa9266Pas encore d'évaluation
- Safer Crystal Meth Smoking: Signs of OverdoseDocument2 pagesSafer Crystal Meth Smoking: Signs of OverdoseCali JeansPas encore d'évaluation
- Appendicitis NCPDocument5 pagesAppendicitis NCPEarl Joseph DezaPas encore d'évaluation
- Appendicitis - NCPDocument5 pagesAppendicitis - NCPEarl Joseph Deza100% (1)
- NCP Acute Pain Related To InflammationDocument3 pagesNCP Acute Pain Related To InflammationMa. Elaine Carla Tating38% (8)
- Pain ManagementDocument29 pagesPain ManagementCrazy StrangerPas encore d'évaluation
- Nursing Care PlanDocument2 pagesNursing Care PlanEden Marie FranciscoPas encore d'évaluation
- Pain Management MidDocument28 pagesPain Management MidPotato PceePas encore d'évaluation
- Nursing Care Plan: Patient Name: James Japitana AGE:28 Sex:Male DiagnosisDocument4 pagesNursing Care Plan: Patient Name: James Japitana AGE:28 Sex:Male DiagnosisGaming BoyPas encore d'évaluation
- Nursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For InfluenzaDocument6 pagesNursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For InfluenzaJinaan MahmudPas encore d'évaluation
- Pain Basic Consideration PDFDocument4 pagesPain Basic Consideration PDFCiprian CorneaPas encore d'évaluation
- Nursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For PharyngitisDocument6 pagesNursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For PharyngitisJinaan MahmudPas encore d'évaluation
- Pi Is 1467298716309412Document10 pagesPi Is 1467298716309412Jonathan ZapataPas encore d'évaluation
- Ketamine For Pain Management.7Document8 pagesKetamine For Pain Management.7Jonathan ZapataPas encore d'évaluation
- Effect of Milk Production On Reproductive Performance in Dairy HerdsDocument10 pagesEffect of Milk Production On Reproductive Performance in Dairy HerdsJonathan ZapataPas encore d'évaluation
- Pogatzki Zahn2017Document16 pagesPogatzki Zahn2017Indra IhsanPas encore d'évaluation
- Corticoadrenal and Cardiorespiratory Responses To Administration of Propofol Combined With Dexmedetomidine or Ketamine in RabbitsDocument4 pagesCorticoadrenal and Cardiorespiratory Responses To Administration of Propofol Combined With Dexmedetomidine or Ketamine in RabbitsJonathan ZapataPas encore d'évaluation
- Corticoadrenal and Cardiorespiratory Responses To Administration of Propofol Combined With Dexmedetomidine or Ketamine in RabbitsDocument4 pagesCorticoadrenal and Cardiorespiratory Responses To Administration of Propofol Combined With Dexmedetomidine or Ketamine in RabbitsJonathan ZapataPas encore d'évaluation
- Corticoadrenal and Cardiorespiratory Responses To Administration of Propofol Combined With Dexmedetomidine or Ketamine in RabbitsDocument4 pagesCorticoadrenal and Cardiorespiratory Responses To Administration of Propofol Combined With Dexmedetomidine or Ketamine in RabbitsJonathan ZapataPas encore d'évaluation
- Evaluación Cardiorrespiratoria de Conejos (Oryctolagus Cuniculus) Anestesiados Con Una Combinación de Tramadol, Acepromacina, Xilazina y KetaminaDocument7 pagesEvaluación Cardiorrespiratoria de Conejos (Oryctolagus Cuniculus) Anestesiados Con Una Combinación de Tramadol, Acepromacina, Xilazina y KetaminaJonathan ZapataPas encore d'évaluation
- ECTOPIC PREGNANCY (POST-OP) CASE COMPILATIONDocument15 pagesECTOPIC PREGNANCY (POST-OP) CASE COMPILATIONmaglaquihermiePas encore d'évaluation
- Ampra Depo UgdDocument2 pagesAmpra Depo UgdCitra NingrumPas encore d'évaluation
- Dafus AgasDocument2 pagesDafus AgasHerawati YustikasariPas encore d'évaluation
- NCP - Acute Pain Related To Presence of Postoperative Surgical IncisionDocument2 pagesNCP - Acute Pain Related To Presence of Postoperative Surgical IncisionRene John Francisco90% (10)
- NaloxBox Press Event Agenda and News ReleaseDocument5 pagesNaloxBox Press Event Agenda and News ReleaseABC6/FOX28Pas encore d'évaluation
- Aspirin Paracetamol CaffeineDocument3 pagesAspirin Paracetamol CaffeineMariusNeicuPas encore d'évaluation
- NSG 318 Teaching AssignmentDocument3 pagesNSG 318 Teaching AssignmentKorena BuffingtonPas encore d'évaluation
- 3 NCPDocument2 pages3 NCPAdreanah Martin RañisesPas encore d'évaluation
- Pri-Med Midwest Full Conference BrochureDocument9 pagesPri-Med Midwest Full Conference BrochurePri-MedPas encore d'évaluation
- Neuromuscular ExerciseDocument10 pagesNeuromuscular ExerciseJuan Fran CoachPas encore d'évaluation
- Wabinga, Shyn Margareth B. Sas 23 Case Study BDocument3 pagesWabinga, Shyn Margareth B. Sas 23 Case Study BShyn MargarethPas encore d'évaluation
- Jurnal Frozen PDFDocument27 pagesJurnal Frozen PDFFahmi MiPas encore d'évaluation
- Medical-Surgical Nursing Pain Management StrategiesDocument5 pagesMedical-Surgical Nursing Pain Management StrategiesMark Russel Sean LealPas encore d'évaluation
- SarafDocument220 pagesSarafAnonymous hF9HwHVuqPas encore d'évaluation
- We-Sol CBT Sample MCQsDocument16 pagesWe-Sol CBT Sample MCQsLip Stick100% (5)
- NCP Pain TeresitoDocument3 pagesNCP Pain TeresitoTheresa Reyes De JesusPas encore d'évaluation
- NCPDocument14 pagesNCPRaidis Pangilinan0% (1)
- Chapter 44 - Connective Tissue DisordersDocument8 pagesChapter 44 - Connective Tissue DisordersStaceyPas encore d'évaluation
- Operant Learning Theory in Pain and Chronic Pain RDocument11 pagesOperant Learning Theory in Pain and Chronic Pain RRhea AquinoPas encore d'évaluation
- Music Therapy and MusicMedicineDocument7 pagesMusic Therapy and MusicMedicineAnjuka100% (1)
- 1000 MCQ Book Pain MedicineDocument215 pages1000 MCQ Book Pain Medicineihtisham1100% (16)
- Total Hip Replacement Rehab ProtocolDocument11 pagesTotal Hip Replacement Rehab ProtocolnurulishtimalPas encore d'évaluation
- Clinical GuidelinesDocument34 pagesClinical GuidelinesAlberto PachecoPas encore d'évaluation
- Acute Pain Nursing Diagnosis & Care Plan - NurseslabsDocument15 pagesAcute Pain Nursing Diagnosis & Care Plan - NurseslabsRena Safitri100% (1)
- How To Set Up A Pain ClinicDocument33 pagesHow To Set Up A Pain ClinicAmhae YunussPas encore d'évaluation
- Ot in Rehab PPT 2Document37 pagesOt in Rehab PPT 2Aarthi ArumugamPas encore d'évaluation
- The Effect of Aromatherapy With Lavender Essence On Severity of Labor Pain and Duration of Labor in Primiparous WomenDocument7 pagesThe Effect of Aromatherapy With Lavender Essence On Severity of Labor Pain and Duration of Labor in Primiparous WomenAini HiolaPas encore d'évaluation
- Chapter 1 PainDocument7 pagesChapter 1 PainMaria ArregoitiaPas encore d'évaluation
- Comparative Evaluation of Passive, Active, and Pasive-Activa DistractionDocument6 pagesComparative Evaluation of Passive, Active, and Pasive-Activa DistractionFernanda BonfilPas encore d'évaluation
- Pt. Indobaruna Bulk Transport: +62-21-297796 +62-21-297796 TLP: / FaxDocument2 pagesPt. Indobaruna Bulk Transport: +62-21-297796 +62-21-297796 TLP: / Faxrabbani aswanPas encore d'évaluation
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryD'EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryPas encore d'évaluation
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionD'EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsD'EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsÉvaluation : 4.5 sur 5 étoiles4.5/5 (6)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryD'EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryÉvaluation : 5 sur 5 étoiles5/5 (47)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildD'EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildÉvaluation : 3.5 sur 5 étoiles3.5/5 (9)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductD'EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductÉvaluation : 5 sur 5 étoiles5/5 (31)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsD'EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsPas encore d'évaluation
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousD'EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousÉvaluation : 5 sur 5 étoiles5/5 (22)
- Little Red Book: Alcoholics AnonymousD'EverandLittle Red Book: Alcoholics AnonymousÉvaluation : 5 sur 5 étoiles5/5 (20)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionD'EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionÉvaluation : 5 sur 5 étoiles5/5 (63)
- Quitting Smoking & Vaping For Dummies: 2nd EditionD'EverandQuitting Smoking & Vaping For Dummies: 2nd EditionPas encore d'évaluation
- Stop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenD'EverandStop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenÉvaluation : 5 sur 5 étoiles5/5 (62)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.D'EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Évaluation : 4 sur 5 étoiles4/5 (7)
- Stop Drinking Now: The original Easyway methodD'EverandStop Drinking Now: The original Easyway methodÉvaluation : 5 sur 5 étoiles5/5 (28)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerD'EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerÉvaluation : 5 sur 5 étoiles5/5 (8)
- Easyway Express: Stop Smoking and Quit E-CigarettesD'EverandEasyway Express: Stop Smoking and Quit E-CigarettesÉvaluation : 5 sur 5 étoiles5/5 (15)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingD'EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingÉvaluation : 5 sur 5 étoiles5/5 (11)
- Recovery 2.0: Move Beyond Addiction and Upgrade Your LifeD'EverandRecovery 2.0: Move Beyond Addiction and Upgrade Your LifeÉvaluation : 5 sur 5 étoiles5/5 (8)
- Healing the Scars of Addiction: Reclaiming Your Life and Moving into a Healthy FutureD'EverandHealing the Scars of Addiction: Reclaiming Your Life and Moving into a Healthy FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (7)
- Blood Orange Night: My Journey to the Edge of MadnessD'EverandBlood Orange Night: My Journey to the Edge of MadnessÉvaluation : 4 sur 5 étoiles4/5 (42)
- Breathing Under Water: Spirituality and the Twelve StepsD'EverandBreathing Under Water: Spirituality and the Twelve StepsÉvaluation : 4.5 sur 5 étoiles4.5/5 (41)
- Guts: The Endless Follies and Tiny Triumphs of a Giant DisasterD'EverandGuts: The Endless Follies and Tiny Triumphs of a Giant DisasterÉvaluation : 4 sur 5 étoiles4/5 (99)
- Summary of Gary Wilson's Your Brain on PornD'EverandSummary of Gary Wilson's Your Brain on PornÉvaluation : 5 sur 5 étoiles5/5 (1)
- The Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingD'EverandThe Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingÉvaluation : 5 sur 5 étoiles5/5 (10)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDD'EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDÉvaluation : 4 sur 5 étoiles4/5 (8)