Académique Documents
Professionnel Documents
Culture Documents
Dynamical analysis reveals strategies to reduce tuberculosis in the Philippines
Transféré par
Jason AlacapaDescription originale:
Titre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Dynamical analysis reveals strategies to reduce tuberculosis in the Philippines
Transféré par
Jason AlacapaDroits d'auteur :
Formats disponibles
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/308199246
A Dynamical Analysis of Tuberculosis in the Philippines
Article · August 2016
CITATION READS
1 49
3 authors:
King James Balasuela Villasin Angelyn Lao
University of Asia and the Pacific De La Salle University
1 PUBLICATION 1 CITATION 22 PUBLICATIONS 81 CITATIONS
SEE PROFILE SEE PROFILE
Eva Rodriguez
University of Asia and the Pacific
4 PUBLICATIONS 6 CITATIONS
SEE PROFILE
Some of the authors of this publication are also working on these related projects:
Mathematics in the Modern World View project
Stochastic Modeling View project
All content following this page was uploaded by Angelyn Lao on 06 April 2017.
The user has requested enhancement of the downloaded file.
ARTICLE
A dynamical analysis of
tuberculosis in the Philippines
King James B. Villasin1, Angelyn R. Lao2, and Eva M. Rodriguez*,1
1
Department of Mathematics, School of Sciences and Engineering, University of Asia and the Pacific,
Pasig City, Philippines
2
Mathematics Department, De La Salle University, Manila, Philippines
T
uberculosis (TB), an infection obtained from KEYWORDS
Mycobacterium, is the fourth leading cause of death
in the Philippines. It remains to be a problem tuberculosis (TB), dynamics analysis, stability analysis,
especially in developing countries, even after prevalence rate, incidence rate, TB control, Philippines
following guidelines and achieving some of the
targets set by the World Health Organization (WHO) for TB INTRODUCTION
elimination. Inspired by the TB transmission model developed
Tuberculosis is the infection of Mycobacterium tuberculosis,
by Trauer et al. (2014), we propose a model for TB transmission
acquired through inhaling and causing infection in the lungs
in the Philippines and validated it using Philippine-based data (NIAID, 2009). There are two main kinds of tuberculosis: latent
for TB incidence and prevalence rates in 2003-2013 (WHO, and active. Latent tuberculosis is the inactive infection in which
2014). Using the Theorem of van den Driessche & Watmough the body’s immune system can only control the growth of the
(2002) we show that our proposed Philippine TB model has a bacteria but cannot eradicate them. This makes the infection
locally asymptotically stable endemic equilibrium, with basic non-contagious and asymptomatic. After latency, active TB can
occur and M. tuberculosis can populate, infect and destroy the
reproduction number R0 = 0.4516 and an unstable free-disease
defense mechanism of the body, making the TB contagious
equilibrium, with R0 = 3.8896. Moreover, our projected (NIAID, 2009). Treatments and drugs have already been
simulations show that improving partial immunity, treatment developed, but these drugs have side effects and the treatment
success, treatment duration and case detection in the Philippines can last for at least 6 months thus, costly and open to possibility
will significantly reduce the TB incidence and prevalence rates. of failure (WHO, 2010b). Moreover, treatment failure could
Interestingly, we found that improving vaccine coverage would result in the development of the multi-drug-resistant TB or
not significantly reduce the projected TB incidence and MDR-TB.
prevalence rates. These results can help the Philippines in
Although the World Health Organization (WHO) and countries
improving its TB programs and develop new strategies to affected by TB have set guidelines and targets for TB
eliminate tuberculosis in the country. elimination, some countries are far from achieving them (WHO,
2014a). The Philippines is one of the TB high-burden countries
and is listed as the 13th highest TB-related death rate, 8th highest
TB incidence, and 7th highest TB prevalence as of 2013 (WHO,
2014a). This paper aims to contribute to the Philippines in its
effort to control TB by understanding its dynamics in the country
*Corresponding author through mathematical modelling.
Email Address: eva.rodriguez@uap.asia
Mathematical modelling of disease transmission is a tool for
Received: January 11, 2016
studying an epidemic and can be used for designing epidemic
Revised: July 12, 2016
control strategies and for predicting the effects of certain
Accepted: August 3, 2016
strategies (Abu-Raddad et al., 2009). We want to make sense out
of the data and provide meaning to the model (Wolkenhauer et
Vol. 10 | No. 01 | 2017 Philippine Science Letters 29
al., 2009). A valid model can be used to project the effects of
interventions made on the dynamics of a disease for short or long
periods. The long-term effects can be determined by looking at
the stability of the system, while the short-term effects are
identified by numerically analyzing the model.
Related studies investigated the impact of strategies on
eliminating TB such as improving case detection, treatment and
vaccination. Trauer et al. (2014) showed that case detection rate
is a sensitive parameter of TB prevalence and mortality. Bhunu
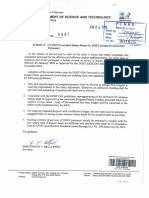
Figure 1. Diagram of our proposed model for TB transmission in the
et al. (2011) highlighted the role of treatment success, arguing Philippines. The population is assumed to be homogeneous and is
that a high case detection rate with low treatment success rate divided into 6 compartments (represented by boxes): the susceptible
could still result in an endemic situation. Moreover, Dowdy and unimmunized group (SA), the susceptible and partially immunized
Chaisson (2009) showed that fixing the treatment success to group (SB), the “slow” latently infected (LA), the “fast” latently infected (LB),
the actively infected and undetected group (I), and the actively infected,
85% will stabilize TB incidence if case detection is less than
detected, and treated (T). Individuals transfer from one group to another
80% although it will decrease yearly only by an average of 1.5% (represented by arrows) with the corresponding rates of transfer
despite rapid case detection increase. They recommended (represented by the parameters indicated on each arrow).
researchers to continuously put efforts to improve case detection
and other factors of TB control, particularly treatment success. In our proposed model (shown in Figure 1), we assumed that the
population is homogeneously mixed and is divided into six (6)
Nainggolan et al. (2013), comparing the TB dynamics with and
groups or compartments: the susceptible unimmunized group S ;
without vaccination, showed that incorporating vaccination A
the susceptible and partially immunized S ; the “slow” latently
significantly lowers the maximum number of latently and B
infected L ; the “fast” latently infected L ; the actively infected
actively infected persons and always reduces the basic A B
and undetected group I; and the actively infected, detected and
reproduction number (average secondary infection caused by an
treated T. The whole population increases by birth with rate (1 −
infectious individual, (van den Driessche and Watmough,
i)Λ + iΛ, where Λ is the constant birth rate and i is the fraction
2002)). Moreover, Lietman and Blower (2000), analysing the
of those who got TB vaccine. The whole population decreases
effects of pre-exposure and post-exposure vaccines on TB
by death: μ is the natural death rate, μ is the death rate of actively
dynamics, showed that if TB incidence is high (greater than 100 i
infected and undetected persons, while μ is the death rate of
per 100,000 population), then the reduction due to post-exposure t
those actively infected and detected.
vaccine is greater than that due to pre-exposure vaccine; and, if
the TB incidence is low, then the reduction due to pre-exposure
Similar to the model of Trauer et al., we assumed frequency-
vaccine is greater. They recommended therefore, that a
dependent transmission. In this case, the unimmunized and
combination of pre-exposure and post-exposure vaccines be
immunized susceptible individuals become infected with the
used to aid in eliminating TB in developing countries. Trauer et #$(& ( )*) -#$(& ( )*)
al. (2014) however, found out that vaccine coverage is not a respective force of infection 𝜆 = and 𝜆d = ,
, ,
sensitive parameter of TB prevalence and mortality. where β is the effective contact rate, 𝜌 is the fraction of those
who are infectious, h is the modification of infectiousness of
How can these results help the Philippines strategize a more those who are treated, and 𝝌 is partial immunity that is either
effective TB control in the country? This paper aims to answer acquired from vaccination or developed from previous TB
this question through mathematical modelling of TB dynamics disease.
in the Philippines. We propose a TB transmission model for the
Philippine setting by modifying the model formulated by Trauer Moreover, our proposed model assumed that the L group could A
et al. (2014) based on the TB incidence and prevalence data for undergo fast progression to active TB at rate ε or slow
the Philippines as reported by the World Health Organization progression and go to L group at rate k. Those in L could
B B
(WHO) for 2003-2013. Our proposed model will be analyzed for develop active TB with rate v, or acquire additional infection and
stability and used to determine factors which can significantly go to “slow” latency group L with force of infection 𝜆 . Those
A d
reduce TB in the country. Conclusions of this study can give who develop active TB but are undetected could be cured
important insights for the development and implementation of without medical treatment at rate 𝛾 or be detected by the national
more effective and efficient TB programs in the Philippines. TB program at rate 𝛿. Those detected are assumed to be treated
immediately. Those who are treated are cured at rate 𝜂𝜑, where
4
THE MODEL 𝜂 is the treatment success rate and is the duration of TB
5
treatment. They could also miss treatment at rate w (default rate).
In this study, we propose a TB transmission model for the
Philippine setting based on the work of Trauer and colleagues All parameters are assumed to be positive since the model only
for the Asia Pacific Region (2014). Restricted by the data that is
deals with positive rates. The values of i, h and 𝜌 range from 0
available for validation, we revised the model of Trauer et al. in
to 1 since they represent ratios. Moreover, since the variables
three ways. First, in order to focus this study only on drug-
represent numbers of individuals, their values are also
susceptible TB, we omitted the drug-resistant compartments in
nonnegative. Given the model in Figure 1, we obtain the
the model. This omission could not significantly affect our study
following system of equations:
since drug-resistant TB in the Philippines is still relatively low
– about 4,000 persons or a prevalence of 4 per 100,000
population as of 2013 (WHO, 2014b). Second, while the model
of Trauer et al. assumed that birth rate is proportional to the total
population, we assumed the birth rate to be constant. This was
done in order to focus the cause of changing population on the
disease. This method of using constant birth rate was also used
by Liu et al. (2011) in their analysis of the TB dynamics in
Guangdong, China. Third, because treatment success rate is an
important element in TB dynamics, we incorporated it in our
model.
30 Philippine Science Letters Vol. 10 | No. 01 | 2017
Parameter subjected to model fitting
Estimated
Effective contact using
β rate 11.5 MatLab
Initial values of the variables
Estimated
proportion of
actively infected WHO
and undetected database
persons as of (WHO,
2003 0.0053028 2015)
Estimated
proportion of
actively infected, WHO
detected and database
treated persons (WHO,
as of 2003 0.0016072 2015)
(24.24/100
0) x
Estimated 82,604,681 WHO
proportion of [average database
constant birth from 2003 (WHO,
rate to 2013] 2015)
Initial values of the varialbes subject to model fitting
Estimated
proportion of
susceptible
unimmunized
persons as of Estimated in
2003 0.04409 MatLab
Estimated
The system has a total of 19 parameters: 13 have fixed proportion of
susceptible
values throughout the study, 5 were tested for significance immunized
and 1 was subjected to data fitting (β). These are listed in persons as of Estimated in
2003 0.4 MatLab
Table 1 with their corresponding values obtained from Estimated
proportion of
literature. ‘fast’ latently
infected persons Estimated in
Table 1. Summary of model parameters with their as of 2003 0.049 MatLab
Estimated
corresponding descriptions, values and sources. proportion of
PARAMETER DESCRIPTION VALUE SOURCE ‘slow’ latently
Fixed parameters infected persons Estimated in
Early 0.129 over (Diel et al., as of 2003 0.5 MatLab
𝜀 progression 23 months 2011)
Transition to late 0.821 over (Blower et
k latency 23 months al., 1996) DATA FITTING
0.075 over (Blower et
v Reactivation 20 years al., 1996)
Spontaneous 0.63 over 3 (Tiemersma We fitted our proposed model with the data of TB incidence and
𝛾 recovery years et al., 2011) prevalence rates in the Philippines. Incidence and prevalence
TB-specific death 0.2647358 (Liu et al.,
𝜇i rate per year 2011) are two of the key indicators of TB burden in a country.
Treated TB- Prevalence is the number of TB cases at a given point in time,
specific death 0.0210358 (Liu et al.,
𝜇t rate per year 2011) while incidence is the number of new and relapse cases of TB
Treatment occurring in a given time period, usually in one year (WHO,
modification of (Cox et al.,
h infectiousness 0.21 2007) 2014b). Incidence here is estimated by dividing the number of
Constant birth 2,192,078 notified cases by the case detection rate (Glaziou et al., 2009),
Λ rate per year
1 over (“Philippines while prevalence is obtained by adding the notified and
67.862 - Life undetected cases. Prevalence and incidence data are usually
years expectancy
[average at birth expressed in proportion to the total population, which in this
Natural death from 2003 2015,” study we shall call prevalence rate and incidence rate. In
𝜇 rate to 2012] 2015)
0.546 WHO order to fit the data into the model therefore, we first converted
[average database the system given by equations (1) − (9) into a dynamical system
Infectious from 2003 (WHO,
𝜌 proportion to 2013] 2015) where the variables are proportions of the total population.
Death rate due to
di TB alone 𝜇−𝜇
i
Hence,
WHO
database
0.0225 per (WHO,
w Default rate year 2015)
By adding equations (1) − (6), we obtained the time
Death rate due to
TB alone during 8,
dt treatment 𝜇−𝜇
t derivative of the total population N, which is given by
Parameters tested for significance 89
(Colditz et
𝝌 Partial immunity 0.49 al., 1994)
Duration of
treating drug- 6 months (WHO, where d = 𝜇 − 𝜇 and d = 𝜇 − 𝜇. From equation (10) we
i i t t
susceptible TB or 0.5 year 2010a) obtained the following non-dimensionalized system of
0.8664 WHO
[average database ODEs:
BCG vaccination from 2003 (WHO,
i rate to 2013] 2015)
0.7
[average
Treatment from 1995 (WHO,
𝜂 success rate to 2012] 2014b)
WHO
database
Case detection 0.45 per (WHO,
𝛿 rate year 2015)
Vol. 10 | No. 01 | 2017 Philippine Science Letters 31
The exact expressions for LA, LB, I, T, SA, SB, in terms only of the
parameters were computed using Mathematica and are found in
Appendix A.
Free-disease Equilibrium
We denoted the free-disease equilibrium as xo = (LAo, LBo, Io, To,
SAo, SBo). In the free-disease state, the system has no infection.
Thus, we have the following formulations for prevalence and Thus, we have
incidence rates, respectively
LAo = LBo = Io = To = 𝜆 = 𝜆d = 0. (Eq. 27)
o o
Solving for SA and SB , we arrived at the free-disease
equilibrium:
4NO 𝚲 O𝚲
𝐱 M = 0,0,0,0, + . (Eq. 28)
Q Q
Using Philippine data for prevalence and incidence rates Endemic Equilibrium
obtained from the World Health Organization Report for 2003
We denoted the endemic equilibrium as x* = (LA*, LB*, I*, T*, SA*,
to 2013 (WHO, 2015), values for parameters obtained from
SB*). To describe the endemic state of the system, we considered
literature, and assuming initial values for 𝐿; , 𝐿= , 𝐼, 𝑇, 𝑆; , 𝑆= the force of infection
we estimated the effective contact rate 𝛽 for the model using
Matlab and found it to be 11.5. All simulations in this paper were #$(& ∗ ( )* ∗ )
𝜆* = . (Eq. 29)
also done in Matlab. ,
As shown in Figure 2, the fitted values follow the same Since N = SA* + SB* + LA* + LB* + I* + T*, equation (29) can be
decreasing behaviour of the actual values of the incidence and expressed as
prevalence rates of TB in the Philippines. The discrepancies are
within the error bars. Hence, we can say that our model is valid 𝜆*SA* + 𝜆*SB* + 𝜆*LA* + 𝜆*LB* + 𝜆*I* + 𝜆*T* − 𝛽𝜌I* −𝛽𝜌hT* = 0.
and is able to describe the TB dynamics in the Philippines, (Eq. 30)
particularly the TB incidence and prevalence rates in the country.
Substituting the expressions for SA*, SB*, LA*, LB*, I* and T* in
terms of 𝜆* and the parameters, equation (30) resulted into a
polynomial equation of the form
𝜆*n + a1𝜆*n−1 + a2𝜆*n−2 + ⋯ + an−1𝜆* + an = 0, (Eq.31)
where n = 4 since we found four (4) roots using Mathematica.
Two of those roots are imaginary, one is zero and one is real.
Please see Appendix B for their exact expressions. Since 𝜆* is
the force of infection during spread of tuberculosis, we only
considered its nonzero real value in the computation of the
Figure 2. Simulations of actual and fitted values of incidence rate endemic equilibrium, found in Appendix C.
(A) and prevalence rate (B) for the years 2003 to 2013. The fitted
values are obtained using the least square method in MatLab. The
fitted values follow the same decreasing behaviour as the actual In this paper, the analysis of an equilibrium point x0, whether the
values and are within the error brackets of the actual values. free-disease equilibrium or the endemic equilibrium, is based on
the basic reproduction number following the method of van den
STABILITY ANALYSIS OF THE MODEL Driessche & Watmough (2002).
We determined the free-disease and endemic equilibrium points Basic Reproduction number R0
and analyzed their stability. To calculate an equilibrium point x ,0 The basic reproduction number R0 is the average secondary
we equated each of the differential equations (1) − (6) to zero infection produced by an infectious individual in a fully
and solved for the respective variables. Thus we have, susceptible population.
Let x = [LA LB I T SA SB]T be the 6 × 1 matrix containing the
number of individuals x in compartment i. Moreover, let F(x)
i
be the 6 × 1 matrix whose entries Fi(x) are the rates of
32 Philippine Science Letters Vol. 10 | No. 01 | 2017
−
appearance of new infectious individuals in the compartment i, In our model, X = {S , S }. Our computations of F(x), V(x), V (x)
S A B
+
and V(x) is the 6 × 1 matrix whose entries V (x) are the rates of i and V (x) showed that conditions 1 to 4 of the Theorem are
transfer of individuals into and out of compartment i. Thus, V (x) i satisfied. Therefore, in order to determine the stability of the
− + +
= V (x) − V (x), where V (x) is the rate of transfer of individuals
i i i free-disease and endemic equilibrium points, we only needed to
−
into compartment i and V (x) is the rate of transfer of individuals i check the respective Jacobian matrices of the original ODE
out of compartment i. Hence, system given by equations (1) – (6), evaluated at each
o
equilibrium point, namely J(x ) and J(x ). Details of *
computations in this section are found in Appendices D, E and
F.
and this gave eigenvalues which all have negative real parts.
Moreover, computing for the basic reproduction number we
obtained R = 3.8896 > 1. By the van den Driessche and
0
Watmough Theorem, this implies that the free-disease
equilibrium point is locally asymptotically unstable.
Similarly, we computed the Jacobian matrix of the system of
ODEs for equations (1) – (6) for the endemic equilibrium x , *
J(x ) and obtained eigenvalues which all have negative real parts.
*
Calculating the basic reproduction number we obtained R = 0
0.4516 < 1. By the van den Driessche and Watmough Theorem,
For any equilibrium point of the system x , we defined matrices 0
this implies that the endemic equilibrium point is locally
F and V to be the respective Jacobian of matrices F(x) and V(x). asymptotically stable.
efg 𝐱 h ekg 𝐱 h
That is, 𝐅 = and 𝐕 = .
eig eig These results – that free-disease equilibrium point is unstable
and the endemic equilibrium point is locally asymptotically
Mathematically, the basic reproduction number R is given by R 0 0 stable – are consistent with the fact that the Philippines continues
−1
= r(FV ), where r is the spectral radius of the next generation to be a TB high-burden country and therefore, its population is
−1 −1
matrix, FV (that is, the greatest eigenvalue of the matrix FV , highly susceptible to tuberculosis. Hence, there has to be an
in absolute value). aggressive program to combat the disease in the country. And
the model proposed in this paper can be used to formulate
Stability of the Equilibrium Points strategies for the nation’s TB programs.
To determine the local asymptotic stability of the equilibrium
points, we used the following theorem: SIMULATIONS
Theorem of van den Driessche and Watmough Projected simulations of the incidence and prevalence rates were
Let x be an equilibrium point of a system ẋ = f(x) and X =
0 S based on our proposed TB model for the Philippines in terms of
{x ≥ 0∣x = 0, i = 1, 2, …, m} be the set of all disease-free
i case detection rate, vaccination coverage, partial immunity,
states. duration of treatment and treatment success rate for the years
2013 to 2023. Assuming the initial conditions LA2013(0), L (0), B
2013
− +
Moreover, let F(x), V(x), V (x) and V (x), as defined above, I (0), T (0), S (0), S (0), and N (0) to be the 2013
2013 2013 A B 2013
2013 2013
satisfy the following assumptions: projected values of the system, we calibrated the case detection
1. If x ≥ 0, then F (x), V (x), V (x) ≥ 0, for i = 1, 2, …, n.
− +
i i i
rate, vaccination coverage, partial immunity, duration of
2. If x = 0, V (x) = 0 for i = 1, 2, …, n.
i i
−
treatment and treatment success rate and simulated the projected
In particular, if x ∈ X then V (x) = 0 for i = 1, 2, …, S i
−
incidence and prevalence rates using default parameter values
m. without any adjustments. These were compared with simulations
of projected incidence and prevalence rates made using the
3. F (x) = 0 if i > m.
i calibrated values of each parameter (as shown in Figures 3 and
4. Both F (x) = 0 and V (x) = 0 if x ∈ X for i = 1, 2, …, m.
+ 4).
i i S
5. If F = 0 for all i, then all the eigenvalues of the Jacobian
i
matrix J(x ) at x have negative real parts.
0 0
Then the equilibrium x is locally asymptotically stable when 0
R ≤ 1 and unstable when R > 1.
0 0
Vol. 10 | No. 01 | 2017 Philippine Science Letters 33
Figure 3. Projected incidence rates from year 2013 to 2023 with
the calibrations of partial immunity (A), vaccine coverage (B),
treatment success rate (C) and treatment duration (D). Graphs
show that improving partial immunity, treatment success and
treatment duration will significantly reduce incidence rate while
improving vaccine coverage will not.
Figure 3 shows the simulations of projected incidence rates for
2013-2023 with the corresponding calibration. It can be
observed that partial immunity (Figure 3A), treatment success
(Figure 3C) and treatment duration (Figure 3D) are parameters
that have significant effects on the projected TB incidence rates.
In Figure 3A, adjusting partial immunity reduces the projected Through the projected simulations therefore, we have shown
TB incidence rate very minimally in the first few years, but the that improving the five parameters results in a decline in the
reduction increases in the long run up to 2023. By improving projected TB incidence and prevalence rates in varying degrees.
treatment success, significant reduction on the projection can be However, the projected TB incidence and prevalence rates are
seen for the first years in Figure 3C. The same behavior can be far from zero even up to 2023. This implies a continuing
observed for the adjustments of treatment duration shown in challenge for eliminating tuberculosis in the Philippines.
Figure 3D. In this case, the difference from the default projection
is enormously greater, causing the TB incidence rate to be close We have shown in our study that the effect of improving partial
to zero. However, TB incidence rate suddenly becomes stable in immunity would only be felt in a distant future. Since improving
the next years up to 2023. This implies that the annual decline in partial immunity will provide TB resistance to more individuals
the TB incidence rates in the long run will become low. Still, the who do not have the active disease yet, this will reduce the
effects of treatment success and duration on the projected TB number of active TB cases in the future. Our results also suggest
incidence rate are significant. that the relevant effect of partial immunity may not be solely due
to vaccination (Figures 3B and 4B), because the partial
In Figure 3B, we observe that improving vaccine coverage does immunity in our model does not only include acquired immunity
not significantly reduce the projected TB incidence but this does from vaccination but also developed immunity from previous
not mean that vaccine coverage is not a relevant factor for TB acquisition of infection.
elimination. Decreasing vaccine coverage down to zero would
significantly increase the projected incidence rate. The results The simulations of prevalence rate with different case detection
only mean that further increase in vaccine coverage would not rate (Figure 4) are consistent with what Trauer et al. (2014),
result in a significant change on the projected TB incidence. Bhunu et al. (2011), Dowdy and Chaisson (2009) have shown in
their studies. That is, improving case detection rate means
Figure 4 shows simulations of the effects on prevalence rate. In lowering the number of contagious individuals infecting the
Figure 4A, we observe that the difference of the projected population.
prevalence rate with partial immunity adjustments from the
default projection is small in the first years, but gradually CONCLUSIONS
becomes greater in the next years. Figure 4C shows that
adjustments of treatment success rate cause a small difference, In this study, we proposed a TB transmission model for the
while adjustments of vaccine coverage cause insignificant Philippines based on the work of Trauer et al. (2014) and
difference in Figure 4B. Projections from case detection rate validated it by fitting the model in the data of the incidence and
adjustments shown in Figure 4E, follow the same behavior as prevalence rates for the Philippines obtained from WHO Report
the projections from the partial immunity, but the effect caused (2014). Using the Theorem of van den Driessche & Watmough
by case detection is greater than by partial immunity. Lastly, (2002), we analysed the dynamics of the model based on the
improving treatment duration causes drastic decrease of TB basic reproduction number R . We obtained a free-disease
0
prevalence in the first two years, and maintains slower but equilibrium which is unstable and an endemic equilibrium which
significant decrease in the next years, as shown in Figure 4D. is locally and asymptotically stable. This implies a continued
challenge to control TB in the Philippines.
In the model simulations of the projected TB incidence and
prevalence rates, we found that improving partial immunity,
treatment success and treatment duration will significantly
34 Philippine Science Letters Vol. 10 | No. 01 | 2017
reduce the projected TB incidence in the Philippines. Whereas, 30(4), 621-636. Doi: 10.1016/j.ccm.2009.08.17.
improving partial immunity, treatment success, treatment Harries, A. D., Hargreaves, N. J., Gausi, F., Kwanjana, J. H., &
duration and case detection will significantly reduce the Salaniponi, F. M. (2001). High early death rate in
projected TB prevalence in the Philippines. Interestingly, our tuberculosis patients in Malawi. The International Journal
model simulations suggest that improving vaccine coverage will of Tuberculosis and Lung Disease: The Official Journal of
not significantly reduce both the TB incidence and prevalence the International Union Against Tuberculosis and Lung
rates. Disease, 5(11), 1000–1005.
ACKNOWLEDGMENTS Lietman, T., & Blower, S.M. (2000). Potential impact of
tuberculosis vaccines as epidemic control agents. Clinical
AL held a research fellowship from De La Salle University and Infectious Diseases: An Official Publication of the Infectious
would like to acknowledge the support of the University’s Diseases Society of America, 30 Suppl 3, S316–322.
Research Coordination Office and CENSER’s Mathematical http://doi.org/10.1086/313881
and Statistical Modeling Unit. The funders had no role in the
design of the study, data collection and analysis, decision to Liu, L., Zhou, Y.&Wu, J. (2008). Global Dynamics in a TB
publish, or preparation of the manuscript. Model Incorporating Case Detection And Two Treatment
Stages. Rocky Mountain Journal of Mathematics - ROCKY
MT J MATH, 38(2008). http://doi.org/10.1216/RMJ-2008-
CONFLICTS OF INTEREST
38-5-1541
There is no conflict of interest among the authors. Liu, Y., Sun, Z., Sun, G., Zhong, Q., Jiang, L., Zhou, L& Jia, Z.
(2011). Modeling Transmission of Tuberculosis with MDR
CONTRIBUTIONS OF INDIVIDUAL AUTHORS and Undetected Cases. Discrete Dynamics in Nature and
Society, 12. http://doi.org/10.1155/2011/296905
KJV performed the modeling and wrote the first draft of the
manuscript. AL and ER supervised the work and contributed to Mathematica. Wolfram.
the writing and editing of the manuscript.
Matlab. MathWorks.
REFERENCES Nainggolan, J., Supian, S., Supriatna, A. K.&Anggriani, N.
(2013). Mathematical Model Of Tuberculosis Transmission
Abu-Raddad, L. J., Sabatelli, L., Achterberg, J. T., Sugimoto, J. With Reccurent Infection And Vaccination. Journal of
D., Longini, I. M., Dye, C., & Halloran, M. E. (2009). Physics, 1–8. http://doi.org/10.1088/1742-
Epidemiological benefits of more-effective tuberculosis 6596/423/1/012059
vaccines, drugs, and diagnostics. Proceedings of the
National Academy of Sciences, 106(33), 13980–13985. NIAID (2009, March 6). Detailed Explanation of TB. Retrieved
http://doi.org/10.1073/pnas.0901720106 April 14, 2015, from
https://www.niaid.nih.gov/topics/tuberculosis/Understandin
Bhunu, C.P., Mushayabasa, S., Magombedze, G.&Roeger, L.I. g/WhatIsTB/pages/detailed.aspx
(2011). Tuberculosis transmission model with case detection
and treatment. Journal of Applied Mathematics and Okuonghae, D., Korobeinikov, A. (2007). Dynamics of
Informatics, 29(3), 529–546. Tuberculosis: The effect of Direct ObservationTherapy
Strategy (DOTS) in Nigeria. Mathematical Modelling of
Colditz, G. A., Brewer, T. F., Berkey, C. S., Wilson, M. E., Natural Phenomena, 2(1), 113–128.
Burdick, E., Fineberg, H. V., & Mosteller, F. (1994). http://doi.org/10.1051/mmnp:2008013
Efficacy of BCG vaccine in the prevention of tuberculosis.
Meta-analysis of the published literature. JAMA, 271(9), Philippines - Life expectancy at birth 2015. (2015, April 18).
698–702. Retrieved April 18, 2015, from
http://countryeconomy.com/demography/life-
Cox, H. S., Niemann, S., Ismailov, G., Doshetov, D., Orozco, J. expectancy/philippines
D., Blok, L., … Kebede, Y. (2007). Risk of Acquired Drug
Resistance during Short-Course Directly Observed Raja, A. (2004). Immunology of tuberculosis. The Indian
Treatment of Tuberculosis in an Area with High Levels of Journal of Medical Research, 120(4), 213–232.
Drug Resistance. Clinical Infectious Diseases, 44(11),
1421–1427. http://doi.org/10.1086/517536 Tiemersma, E. W., van der Werf, M. J., Borgdorff, M. W.,
Diel, R., Loddenkemper, R., Niemann, S., Meywald-Walter, K., Williams, B. G., & Nagelkerke, N. J. D. (2011). Natural
& Nienhaus, A. (2011). Negative and positive predictive history of tuberculosis: duration and fatality of untreated
value of a whole-blood interferon-γ release assay for pulmonary tuberculosis in HIV negative patients: a
developing active tuberculosis: an update. American Journal systematic review. PloS One, 6(4), e17601.
of Respiratory and Critical Care Medicine, 183(1), 88–95. http://doi.org/10.1371/journal.pone.0017601
http://doi.org/10.1164/rccm.201006-0974OC
Trauer, J. M., Denholm, J. T., & McBryde, E. S. (2014).
Dowdy, D. W., & Chaisson, R. E. (2009). The persistence of Construction of a mathematical model for tuberculosis
tuberculosis in the age of DOTS: reassessing the effect of transmission in highly endemic regions of the Asia-pacific.
case detection. Bulletin of the World Health Organization, Journal of Theoretical Biology, 358, 74–84.
87(4), 296–304. http://doi.org/10.1016/j.jtbi.2014.05.023
Glaziou, P., Floyd, K. and Raviglione, M. (2009). Global Van den Driessche, P., & Watmough, J. (2002). Reproduction
Burden and Epidemiology of Tuberculosis. Clin Chest Med, numbers and sub-threshold endemic equilibria for
Vol. 10 | No. 01 | 2017 Philippine Science Letters 35
compartmental models of disease transmission.
Mathematical Biosciences, 180, 29–48.
WHO. (2014a). Global Tuberculosis Report. Geneva,
Switzerland.
WHO (2014b). Reported estimates of BCG coverage.Retrieved
April 18, 2015, from
http://apps.who.int/immunization_monitoring/globalsumm
ary/timeseries/tscoveragebcg.html
WHO (2015). WHO | Download data as CSV files.Retrieved
April 18, 2015, from
http://www.who.int/tb/country/data/download/en/
Wolkenhauer, O., Lao, A., Omholt, S., & Martens, H. (2009).
Systems approaches in molecular and cell biology: making
sense out of data and providing meaning to models. In Proc.
SPIE 7343, Independent Component Analyses, Wavelets,
Neural Networks, Biosystems, and Nanoengineering VII
(Vol. 7343, p. 734318). http://doi.org/10.1117/12.822742
36 Philippine Science Letters Vol. 10 | No. 01 | 2017
Appendix A: Equilibrium points for the system of ODEs given by Eqns (1) − (6)
Solve x0 = [LA0, LB0, I0, T0, SA0, SB0]
To solve for the equilibrium points x0, we set each of the differential equations (1) − (6) to 0 and compute for [LA0, LB0, I0, T0, SA0, SB0]. In
the following computations, these are expressed as [L1, L2, I1, T, S1, S2] respectively. Also, 𝜇1 and 𝜇2 corresponds to 𝜇i and 𝜇t,
respectively.
We arrive at the following solutions:
S2 → − −i k w 𝛾 𝜆 𝚲 𝜇 − i w 𝛾 ϵ 𝜆 𝚲 𝜇 − i k w 𝛾 𝚲 𝜇2 − i w 𝛾 ϵ 𝚲 𝜇2 − i w 𝛾 𝜆 𝚲 𝜇2 − i w 𝛾 𝚲 𝜇3 − i k v w 𝜆 𝚲 𝜇1 −
i v w ϵ 𝜆 𝚲 𝜇1 − i k v w 𝚲 𝜇 𝜇1 − i v w ϵ 𝚲 𝜇 𝜇1 − i k w 𝜆 𝚲 𝜇 𝜇1 − i v w 𝜆 𝚲 𝜇 𝜇1 − i w ϵ 𝜆 𝚲 𝜇 𝜇1 −
i k w 𝚲 𝜇2 𝜇1 − i v w 𝚲 𝜇2 𝜇1 − i w ϵ 𝚲 𝜇2 𝜇1 − i w 𝜆 𝚲 𝜇2 𝜇1 − i w 𝚲 𝜇3 𝜇1 − i k v 𝛿 𝜆 𝚲 𝜇2 − i v 𝛿 ϵ 𝜆 𝚲 𝜇2 −
i k v 𝛿 𝚲 𝜇 𝜇2 − i v 𝛿 ϵ 𝚲 𝜇 𝜇2 − i k 𝛾 𝜆 𝚲 𝜇 𝜇2 − i v 𝛿 𝜆 𝚲 𝜇 𝜇2 − i 𝛾 ϵ 𝜆 𝚲 𝜇 𝜇2 −
i 𝛿 ϵ 𝜆 𝚲 𝜇 𝜇2 − i k 𝛾 𝚲 𝜇2 𝜇2 − i k 𝛿 𝚲 𝜇2 𝜇2 − i v 𝛿 𝚲 𝜇2 𝜇2 − i 𝛾 ϵ 𝚲 𝜇2 𝜇2 − i 𝛿 ϵ 𝚲 𝜇2 𝜇2 − i 𝛾 𝜆 𝚲 𝜇2 𝜇2 −
i 𝛿 𝜆 𝚲 𝜇2 𝜇2 − i 𝛾 𝚲 𝜇3 𝜇2 − i 𝛿 𝚲 𝜇3 𝜇2 − i k v 𝜆 𝚲 𝜇1 𝜇2 − i v ϵ 𝜆 𝚲 𝜇1 𝜇2 − i k v 𝚲 𝜇 𝜇1 𝜇2 −
i v ϵ 𝚲 𝜇 𝜇1 𝜇2 − i k 𝜆 𝚲 𝜇 𝜇1 𝜇2 − i v 𝜆 𝚲 𝜇 𝜇1 𝜇2 − i ϵ 𝜆 𝚲 𝜇 𝜇1 𝜇2 − i k 𝚲 2% 𝜇1 𝜇2 − i v 𝚲 𝜇2 𝜇1 𝜇2 −
i ϵ 𝚲 𝜇2 𝜇1 𝜇2 − i 𝜆 𝚲 𝜇2 𝜇1 𝜇2 − i 𝚲 𝜇3 𝜇1 𝜇2 − k v 𝛿 𝜂 𝜆 𝚲 𝜙 − v 𝛿 ϵ 𝜂 𝜆 𝚲 𝜙 − i k v 𝛿 𝜂 𝚲 𝜇 𝜙 −
iv𝛿ϵ𝜂𝚲𝜇𝜙−ik𝛾𝜂𝜆𝚲𝜇𝜙−ik𝛿𝜂𝜆𝚲𝜇𝜙−iv𝛿𝜂𝜆𝚲𝜇𝜙−i𝛾ϵ𝜂𝜆𝚲𝜇𝜙−𝛿ϵ𝜂𝜆𝚲𝜇𝜙−
i k 𝛾 𝜂 𝚲 𝜇2 𝜙 − i k 𝛿 𝜂 𝚲 𝜇2 𝜙 − i v 𝛿 𝜂 𝚲 𝜇2 𝜙 − i 𝛾 ϵ 𝜂 𝚲 𝜇2 𝜙 − i 𝛿 ϵ 𝜂 𝚲 𝜇2 𝜙 − i 𝛾 𝜂 𝜆 𝚲 𝜇2 𝜙 −
i 𝛿 𝜂 𝜆 𝚲 𝜇2 𝜙 − i 𝛾 𝜂 𝚲 𝜇3 𝜙 − i 𝛿 𝜂 𝚲 𝜇3 𝜙 − i k v 𝜂 𝜆 𝚲 𝜇1 𝜙 − i v ϵ 𝜂 𝜆 𝚲 𝜇1 𝜙 − i k v 𝜂 𝚲 𝜇 𝜇1 𝜙 −
i v ϵ 𝜂 𝚲 𝜇 𝜇1 𝜙 − i k 𝜂 𝜆 𝚲 𝜇 𝜇1 𝜙 − i v 𝜂 𝜆 𝚲 𝜇 𝜇1 𝜙 − i ϵ 𝜂 𝜆 𝚲 𝜇 𝜇1 𝜙 − i k 𝜂 𝚲 𝜇2 𝜇1 𝜙 − i v 𝜂 𝚲 𝜇2 𝜇1 𝜙 −
i ϵ 𝜂 𝚲 𝜇2 𝜇1 𝜙 − i 𝜂 𝜆 𝚲 𝜇2 𝜇1 𝜙 − i 𝜂 & 𝜇3 𝜇1 𝜙 − i w 𝛾 𝜆2 𝚲 𝜇𝝌 − i w 𝛾 𝜆 𝚲 𝜇2 𝝌 − i w ϵ 𝜆2 𝚲 𝜇1 𝝌 −
i w ϵ 𝜆 𝚲 𝜇 𝜇1 𝝌 − i w 𝜆2 𝚲 𝜇 𝜇1 𝝌 − i w 𝜆 𝚲 𝜇2 𝜇1 𝝌 − i 𝛿 ϵ 𝜆2 𝚲 𝜇2 𝝌 − i 𝛿 ϵ 𝜆 𝚲 𝜇 𝜇2 𝝌 − i 𝛾 𝜆2 𝚲 𝜇 𝜇2 𝝌 −
i 𝛿 𝜆2 𝚲 𝜇 𝜇2 𝝌 − i 𝛾 𝜆 𝚲 𝜇2 𝜇2 𝝌 − i 𝛿 𝜆 𝚲 𝜇2 𝜇2 𝝌 − i ϵ 𝜆2 𝚲 𝜇1 𝜇2 𝝌 − i ϵ 𝜆 𝚲 𝜇 𝜇1 𝜇2 𝝌 − i 𝜆2 𝚲 𝜇 𝜇1 𝜇2 𝝌 −
i 𝜆 𝚲 𝜇2 𝜇1 𝜇2 𝝌 − 𝛿 ϵ 𝜂 𝜆2 𝚲 𝜙 𝝌 − i 𝛿 ϵ 𝜂 𝜆 𝚲 𝜇 𝜙 𝝌 − i 𝛾 𝜂 𝜆2 𝚲 𝜇 𝜙 𝝌 − i 𝛿 𝜂 𝜆2 𝚲 𝜇 𝜙 𝝌 − i 𝛾 𝜂 𝜆 𝚲 𝜇2 𝜙 𝝌 −
i 𝛿 𝜂 𝜆 𝚲 𝜇2 𝜙 𝝌 − i ϵ 𝜂 𝜆2 𝚲 𝜇1 𝜙 𝝌 − i ϵ 𝜂 𝜆 𝚲 𝜇 𝜇1 𝜙 𝝌 − i 𝜂 𝜆2 𝚲 𝜇 𝜇1 𝜙 𝝌 − i 𝜂 𝜆 𝚲 𝜇2 𝜇1 𝜙 𝝌
(𝜆 + 𝜇) k w 𝛾 𝜇2 + w 𝛾 ϵ 𝜇2 + w 𝛾 𝜇3 + k v w 𝜇 𝜇1 + v w ϵ 𝜇 𝜇1 + k w 𝜇2 𝜇1 + v w 𝜇2 𝜇1 + w ϵ 𝜇2 𝜇1 +
w 𝜇3 𝜇1 + k v 𝛿 𝜇 𝜇2 + v 𝛿 ϵ 𝜇 𝜇2 + k 𝛾 𝜇2 𝜇2 + k 𝛿 𝜇2 𝜇2 + v 𝛿 𝜇2 𝜇2 + 𝛾 ϵ 𝜇2 𝜇2 + 𝛿 ϵ 𝜇2 𝜇2 +
𝛾 𝜇3 𝜇2 + 𝛿 𝜇3 𝜇2 + k v 𝜇 𝜇1 𝜇2 + v ϵ 𝜇 𝜇1 𝜇2 + k 𝜇2 𝜇1 𝜇2 + v 𝜇2 𝜇1 𝜇2 + ϵ 𝜇2 𝜇1 𝜇2 + 𝜇3 𝜇1 𝜇2 +
k v 𝛿 𝜂 𝜇 𝜙 + v 𝛿 ϵ 𝜂 𝜇 𝜙 + k 𝛾 𝜂 𝜇2 𝜙 + k 𝛿 𝜂 𝜇2 𝜙 + v 𝛿 𝜂 𝜇2 𝜙 + 𝛾 ϵ 𝜂 𝜇2 𝜙 + 𝛿 ϵ 𝜂 𝜇2 𝜙 + 𝛾 𝜂 𝜇3 𝜙 +
𝛿 𝜂 𝜇3 𝜙 + k v 𝜂 𝜇 𝜇1 𝜙 + v ϵ 𝜂 𝜇 𝜇1 𝜙 + k 𝜂 𝜇2 𝜇1 𝜙 + v 𝜂 𝜇2 𝜇1 𝜙 + ϵ 𝜂 𝜇2 𝜇1 𝜙 + 𝜂 𝜇3 𝜇1 𝜙 +
k w 𝛾 𝜆 𝜇 𝝌 + w 𝛾 ϵ 𝜆 𝜇 𝝌 + 2 w 𝛾 𝜆 𝜇2 𝝌 + k v w 𝜆 𝜇1 𝝌 + v w ϵ 𝜆 𝜇1 𝝌 + k w 𝜆 𝜇 𝜇1 𝝌 + v w 𝜆 𝜇 𝜇1 𝝌 +
2 w ϵ 𝜆 𝜇 𝜇1 𝝌 + 2 w 𝜆 𝜇2 𝜇1 𝝌 + k v 𝛿 𝜆 𝜇2 𝝌 + v 𝛿 ϵ 𝜆 𝜇2 𝝌 + k 𝛾 𝜆 𝜇 𝜇2 𝝌 + k 𝛿 𝜆 𝜇 𝜇2 𝝌 +
v 𝛿 𝜆 𝜇 %2 𝝌 + 𝛾 ϵ 𝜆 𝜇 𝜇2 𝝌 + 2 𝛿 ϵ 𝜆 𝜇 𝜇2 𝝌 + 2 𝛾 𝜆 𝜇2 𝜇2 𝝌 + 2 𝛿 𝜆 𝜇2 𝜇2 𝝌 + k v 𝜆 𝜇1 𝜇2 𝝌 +
v ϵ 𝜆 𝜇1 𝜇2 𝝌 + k 𝜆 𝜇 𝜇1 𝜇2 𝝌 + v 𝜆 𝜇 𝜇1 𝜇2 𝝌 + 2 ϵ 𝜆 𝜇 𝜇1 𝜇2 𝝌 + 2 𝜆 𝜇2 𝜇1 𝜇2 𝝌 + k 𝛾 𝜂 𝜆 𝜇 𝜙 𝝌 +
k 𝛿 𝜂 𝜆 𝜇 ' 𝝌 + v 𝛿 𝜂 𝜆 𝜇 𝜙 𝝌 + 𝛾 ϵ 𝜂 𝜆 𝜇 𝜙 𝝌 + 𝛿 ϵ 𝜂 𝜆 𝜇 𝜙 𝝌 + 2 𝛾 𝜂 𝜆 𝜇2 𝜙 𝝌 + 2 𝛿 𝜂 𝜆 𝜇2 𝜙 𝝌 +
k v 𝜂 𝜆 𝜇1 𝜙 𝝌 + v ϵ 𝜂 𝜆 𝜇1 𝜙 𝝌 + k 𝜂 𝜆 𝜇 𝜇1 𝜙 𝝌 + v 𝜂 𝜆 𝜇 𝜇1 𝜙 𝝌 + 2 ϵ 𝜂 𝜆 𝜇 𝜇1 𝜙 𝝌 + 2 𝜂 𝜆 𝜇2 𝜇1 𝜙 𝝌 +
w 𝛾 𝜆2 𝜇 𝝌2 + w ϵ 𝜆2 𝜇1 𝝌2 + w 𝜆2 𝜇 𝜇1 𝝌2 + 𝛿 ϵ 𝜆2 𝜇2 𝝌2 + 𝛾 𝜆2 𝜇 𝜇2 𝝌2 + 𝛿 𝜆2 𝜇 𝜇2 𝝌2 +
ϵ 𝜆2 𝜇1 𝜇2 𝝌2 + 𝜆2 𝜇 𝜇1 𝜇2 𝝌2 + 𝛾 𝜂 𝜆2 𝜇 𝜙 𝝌2 + 𝛿 𝜂 𝜆2 𝜇 𝜙 𝝌2 + ϵ 𝜂 𝜆2 𝜇1 𝜙 𝝌2 + 𝜂 𝜆2 𝜇 𝜇1 𝜙 𝝌2 ,
L1 → 𝜆 𝚲 𝜇 − i 𝜆 𝚲 𝜇 + 𝜆2 𝚲 𝝌 + i 𝜆 𝚲 𝜇 𝝌 (w 𝛾 𝜇 + v w 𝜇1 + w 𝜇 𝜇1 + v 𝛿 𝜇2 + 𝛾 𝜇 𝜇2 + 𝛿 𝜇 𝜇2 +
v 𝜇1 𝜇2 + 𝜇 𝜇1 𝜇2 + v 𝛿 𝜂 𝜙 + 𝛾 𝜂 𝜇 𝜙 + 𝛿 𝜂 𝜇 𝜙 + v 𝜂 𝜇1 𝜙 + 𝜂 𝜇 𝜇1 𝜙 + w 𝛾 𝜆 𝝌 +
w 𝜆 𝜇1 𝝌 + 𝛾 𝜆 𝜇2 𝝌 + 𝛿 𝜆 𝜇 2 𝝌 + 𝜆 𝜇1 𝜇 2 𝝌 + 𝛾 𝜂 𝜆 𝜙 𝝌 + 𝛿 𝜂 𝜆 𝜙 𝝌 + 𝜂 𝜆 𝜇1 𝜙 𝝌)
(𝜆 + 𝜇) k w 𝛾 𝜇2 + w 𝛾 ϵ 𝜇2 + w 𝛾 𝜇3 + k v w 𝜇 𝜇1 + v w ϵ 𝜇 𝜇1 + k w 𝜇2 𝜇1 + v w 𝜇2 𝜇1 + w ϵ 𝜇2 𝜇1 +
w 𝜇3 𝜇1 + k v 𝛿 𝜇 𝜇2 + v 𝛿 ϵ 𝜇 𝜇2 + k 𝛾 𝜇2 𝜇2 + k 𝛿 𝜇2 𝜇2 + v 𝛿 𝜇2 𝜇2 + 𝛾 ϵ 𝜇2 𝜇2 + 𝛿 ϵ 𝜇2 𝜇2 + 𝛾 𝜇3 𝜇2 +
𝛿 𝜇3 𝜇2 + k v 𝜇 𝜇1 𝜇2 + v ϵ 𝜇 𝜇1 𝜇2 + k 𝜇2 𝜇1 𝜇2 + v 𝜇2 𝜇1 𝜇2 + ϵ 𝜇2 𝜇1 𝜇2 + 𝜇3 𝜇1 𝜇2 + k v 𝛿 𝜂 𝜇 𝜙 +
v 𝛿 ϵ 𝜂 𝜇 𝜙 + k 𝛾 𝜂 𝜇2 𝜙 + k 𝛿 𝜂 𝜇2 𝜙 + v 𝛿 𝜂 𝜇2 𝜙 + 𝛾 ϵ 𝜂 𝜇2 𝜙 + 𝛿 ϵ 𝜂 𝜇2 𝜙 + 𝛾 𝜂 𝜇3 𝜙 + 𝛿 𝜂 𝜇3 𝜙 + k v 𝜂 𝜇 𝜇1 𝜙 +
v ϵ 𝜂 𝜇 𝜇1 𝜙 + k 𝜂 𝜇2 𝜇1 𝜙 + v 𝜂 𝜇2 𝜇1 𝜙 + ϵ 𝜂 𝜇2 𝜇1 𝜙 + 𝜂 𝜇3 𝜇1 𝜙 + k w 𝛾 𝜆 𝜇 𝝌 + w 𝛾 ϵ 𝜆 𝜇 𝝌 + 2 w 𝛾 𝜆 𝜇2 𝝌 +
k v w 𝜆 𝜇1 𝝌 + v w ϵ 𝜆 𝜇1 𝝌 + k w 𝜆 𝜇 𝜇1 𝝌 + v w 𝜆 𝜇 𝜇1 𝝌 + 2 w ϵ 𝜆 𝜇 𝜇1 𝝌 + 2 w 𝜆 𝜇2 𝜇1 𝝌 + k v 𝛿 𝜆 𝜇2 𝝌 +
v 𝛿 ϵ 𝜆 𝜇2 𝝌 + k 𝛾 𝜆 𝜇 𝜇2 𝝌 + k 𝛿 𝜆 𝜇 𝜇2 𝝌 + v 𝛿 𝜆 𝜇 𝜇2 𝝌 + 𝛾 ϵ 𝜆 𝜇 𝜇2 𝝌 + 2 𝛿 ϵ 𝜆 𝜇 𝜇2 𝝌 + 2 𝛾 𝜆 𝜇2 𝜇2 𝝌 +
2 𝛿 𝜆 𝜇2 𝜇2 𝝌 + k v 𝜆 𝜇1 𝜇2 𝝌 + v ϵ 𝜆 𝜇1 𝜇2 𝝌 + k 𝜆 𝜇 𝜇1 𝜇2 𝝌 + v 𝜆 𝜇 𝜇1 𝜇2 𝝌 + 2 ϵ 𝜆 𝜇 𝜇1 𝜇2 𝝌 +
2 𝜆 𝜇2 𝜇1 𝜇2 𝝌 + k 𝛾 𝜂 𝜆 𝜇 𝜙 𝝌 + k 𝛿 𝜂 𝜆 𝜇 𝜙 𝝌 + v 𝛿 𝜂 𝜆 𝜇 𝜙 𝝌 + 𝛾 ϵ 𝜂 𝜆 𝜇 𝜙 𝝌 + 𝛿 ϵ ( 𝜆 𝜇 𝜙 𝝌 + 2 𝛾 𝜂 𝜆 𝜇2 𝜙 𝝌 +
2 𝛿 𝜂 𝜆 𝜇2 𝜙 𝝌 + k v 𝜂 𝜆 𝜇1 𝜙 𝝌 + v ϵ 𝜂 𝜆 𝜇1 𝜙 𝝌 + k 𝜂 𝜆 𝜇 𝜇1 𝜙 𝝌 + v 𝜂 𝜆 𝜇 𝜇1 𝜙 𝝌 + 2 ϵ 𝜂 𝜆 𝜇 𝜇1 𝜙 𝝌 +
2 𝜂 𝜆 𝜇2 𝜇1 𝜙 𝝌 + w 𝛾 𝜆2 𝜇 𝝌2 + w ϵ 𝜆2 𝜇1 𝝌2 + w 𝜆2 𝜇 𝜇1 𝝌2 + 𝛿 ϵ 𝜆2 𝜇2 𝝌2 + 𝛾 𝜆2 𝜇 𝜇2 𝝌2 + 𝛿 𝜆2 𝜇 𝜇2 𝝌2 +
ϵ 𝜆2 𝜇1 𝜇2 𝝌2 + 𝜆2 𝜇 𝜇1 𝜇2 𝝌2 + 𝛾 𝜂 𝜆2 𝜇 𝜙 𝝌2 + 𝛿 𝜂 𝜆2 𝜇 𝜙 𝝌2 + ϵ 𝜂 𝜆2 𝜇1 𝜙 𝝌2 + 𝜂 𝜆2 𝜇 𝜇1 𝜙 𝝌2 ,
Vol. 10 | No. 01 | 2017 Philippine Science Letters 37
View publication stats
Vous aimerez peut-être aussi
- Revised Provisional NTPS 2016 Technical Report With Foreword - 20nov2017Document158 pagesRevised Provisional NTPS 2016 Technical Report With Foreword - 20nov2017Jason AlacapaPas encore d'évaluation
- Tangcharoensathien 2018 - Health Systems Development in Thailand - A Solid Platform For Successful Implementation of Universal Health CoverageDocument19 pagesTangcharoensathien 2018 - Health Systems Development in Thailand - A Solid Platform For Successful Implementation of Universal Health CoverageJason AlacapaPas encore d'évaluation
- Articles: BackgroundDocument9 pagesArticles: BackgroundJason AlacapaPas encore d'évaluation
- Universal Health Care PhilippinesDocument47 pagesUniversal Health Care PhilippinesJason AlacapaPas encore d'évaluation
- HSG Annual Report 2017Document16 pagesHSG Annual Report 2017Jason AlacapaPas encore d'évaluation
- DOST Salary Rates 2019Document3 pagesDOST Salary Rates 2019Jason Alacapa71% (14)
- Stenberg 2017 - Financing Transformative Health Systems Towards Achievement of The Health Sustainable Development Goals - A Model For Projected ResourceDocument13 pagesStenberg 2017 - Financing Transformative Health Systems Towards Achievement of The Health Sustainable Development Goals - A Model For Projected ResourceJason AlacapaPas encore d'évaluation
- HSG Annual Report 2017Document16 pagesHSG Annual Report 2017Jason AlacapaPas encore d'évaluation
- USAID & MEASURE Evaluation (2019) - Guide To Fundamentals of Economic Evaluation in Public HealthDocument114 pagesUSAID & MEASURE Evaluation (2019) - Guide To Fundamentals of Economic Evaluation in Public HealthJason AlacapaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- An Introduction To Numerical Methods UsiDocument415 pagesAn Introduction To Numerical Methods UsiChristian Ismaël Tcheutchoua TakamPas encore d'évaluation
- Marker-And-Cell (MAC) Method ExplainedDocument4 pagesMarker-And-Cell (MAC) Method Explainedsurendra ratrePas encore d'évaluation
- KCET 2020 Previous Year Question Paper for Maths - Free PDF DownloadDocument21 pagesKCET 2020 Previous Year Question Paper for Maths - Free PDF Downloaditsmerana326Pas encore d'évaluation
- Cambridge International AS & A Level: Further Mathematics 9231/13Document16 pagesCambridge International AS & A Level: Further Mathematics 9231/13Krrish KhanthPas encore d'évaluation
- Vector Field: Vector Fields On Subsets of Euclidean SpaceDocument8 pagesVector Field: Vector Fields On Subsets of Euclidean SpaceDiego VillalobosPas encore d'évaluation
- Mechanical Behavior of Materials 01 PDFDocument54 pagesMechanical Behavior of Materials 01 PDFjunee100% (2)
- EP 222: Classical Mechanics - Lecture 1: Dipan K. GhoshDocument12 pagesEP 222: Classical Mechanics - Lecture 1: Dipan K. GhoshSiddharth Hari NairPas encore d'évaluation
- Worksheet 5.6 Hinge TheoremDocument2 pagesWorksheet 5.6 Hinge TheoremJho-Ann40% (5)
- THL - 1 - Ece 4600Document21 pagesTHL - 1 - Ece 4600Juju JantonPas encore d'évaluation
- Amf4 PK1Document8 pagesAmf4 PK1Samion AwaldinPas encore d'évaluation
- Laplace Transforms Part IIDocument24 pagesLaplace Transforms Part IIThotakuri Sai Amith ChowdaryPas encore d'évaluation
- 2021 The PondsDocument14 pages2021 The PondsMUBASHIR HUSSAINPas encore d'évaluation
- Preliminary OWR 2018 11Document29 pagesPreliminary OWR 2018 11Jaweria AmjadPas encore d'évaluation
- Integration and Its ApplicationsDocument17 pagesIntegration and Its ApplicationsNooreldeenPas encore d'évaluation
- Jacob Bernoulli's Contributions to Statistics and the Law of Large NumbersDocument2 pagesJacob Bernoulli's Contributions to Statistics and the Law of Large NumbersYvaine MehPas encore d'évaluation
- Empirical Wavelet TransformDocument97 pagesEmpirical Wavelet TransformChristo Jacob KPas encore d'évaluation
- Stochastic Processes and The Mathematics of Finance: Jonathan Block April 1, 2008Document132 pagesStochastic Processes and The Mathematics of Finance: Jonathan Block April 1, 2008.cadeau01Pas encore d'évaluation
- MA8451 Probability and Random ProcessesDocument92 pagesMA8451 Probability and Random ProcessesSujitha SujiPas encore d'évaluation
- System Identification MatlabDocument167 pagesSystem Identification Matlabkarlg100% (1)
- Board Exam Review Schedule April 2018 EE SubjectsDocument1 pageBoard Exam Review Schedule April 2018 EE SubjectsJamesdomingoPas encore d'évaluation
- Polynomials: Created by T. MadasDocument29 pagesPolynomials: Created by T. MadasTanzimPas encore d'évaluation
- Circles, Secants & TangentsDocument39 pagesCircles, Secants & TangentsKimmy Airam Ramos100% (1)
- Class 12 Formula in A3Document20 pagesClass 12 Formula in A3Tshering TashiPas encore d'évaluation
- XII Matrices AssignmentDocument3 pagesXII Matrices AssignmentCRPF SchoolPas encore d'évaluation
- Geometry QuesDocument1 pageGeometry QuesZoe Wang WeiqiPas encore d'évaluation
- Kriging Method and ApplicationDocument56 pagesKriging Method and Applicationsisi100% (1)
- Maxima Book Chapter 9Document64 pagesMaxima Book Chapter 9prakush_prakushPas encore d'évaluation
- UWCABook PDFDocument506 pagesUWCABook PDFDeonisis VersolaPas encore d'évaluation
- TARAY - Laboratory Experiment 7 Matrix AnalysisDocument8 pagesTARAY - Laboratory Experiment 7 Matrix AnalysisFEOLO RIEL BENITEZ TARAYPas encore d'évaluation
- Diverg and Maxwell's First EqDocument16 pagesDiverg and Maxwell's First EqBilal AhmedPas encore d'évaluation