Vous aimerez peut-être aussi
- Galler Spacing Technique (GST) ManualDocument44 pagesGaller Spacing Technique (GST) ManualDavid Galler100% (1)
- DOH Memo No. 2019-0112 New and Renewal ApplicationDocument5 pagesDOH Memo No. 2019-0112 New and Renewal ApplicationMenGuitar100% (3)
- FAQs For Health FacilitiesDocument17 pagesFAQs For Health FacilitiesPhilhealth ISDH SinaitPas encore d'évaluation
- Blank MoaDocument3 pagesBlank MoaGary Arlene YalungPas encore d'évaluation
- Ao2023 0009 PDFDocument54 pagesAo2023 0009 PDFJohn Philip TiongcoPas encore d'évaluation
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayPas encore d'évaluation
- Weekly Notifiable 2023Document1 pageWeekly Notifiable 2023johnmorts2014100% (1)
- Letter of Intent DOHDocument1 pageLetter of Intent DOHVangie Salvacion50% (2)
- DOH Hospital Star Awards 2022 Application GuidelinesDocument2 pagesDOH Hospital Star Awards 2022 Application GuidelinesChang Gelvoleo100% (2)
- Animal Bite FlowchartDocument1 pageAnimal Bite FlowchartBdh AbtcPas encore d'évaluation
- MOA Red CrossDocument4 pagesMOA Red Crossagelesswap100% (2)
- Formulary InclusionDocument11 pagesFormulary InclusionLhye CarmonaPas encore d'évaluation
- Doh Infection Prevention & Control Training Manual: Volume II For Health Facility AdministratorsDocument119 pagesDoh Infection Prevention & Control Training Manual: Volume II For Health Facility AdministratorsAlex SanchezPas encore d'évaluation
- Policies, Standards Requirements For Licensing Birthing ClinicDocument46 pagesPolicies, Standards Requirements For Licensing Birthing ClinicMatt Lao Dionela83% (24)
- CS Form No. 212 Attachment Work Experience Sheet RONADocument2 pagesCS Form No. 212 Attachment Work Experience Sheet RONAKeirl John Asingua100% (1)
- Hemodialysis Patient's Endorsement FormDocument1 pageHemodialysis Patient's Endorsement FormHacienda Galea Resort and Events Place100% (1)
- Assessment Tool For Licensing A General Clinical Lab New AoDocument19 pagesAssessment Tool For Licensing A General Clinical Lab New AoCmm Michael De Silva100% (1)
- 2019-IPCR - HRH Nurse Midwife Dentist Pharma MedtechDocument29 pages2019-IPCR - HRH Nurse Midwife Dentist Pharma MedtechKarina Santos100% (8)
- Members DirectoryDocument32 pagesMembers DirectoryMicheal J Jacson100% (1)
- Critical Thinking ActivitiesDocument2 pagesCritical Thinking ActivitiesSaba BaigPas encore d'évaluation
- ASAM 101: How To Complete The ASAM Placement FormDocument24 pagesASAM 101: How To Complete The ASAM Placement FormMistor Dupois Williams100% (2)
- Doh Ihmop Filled UpDocument12 pagesDoh Ihmop Filled UpRex Quilla100% (1)
- PDR - 03072014 Philhealth Form PDFDocument1 pagePDR - 03072014 Philhealth Form PDFMARY ANGELIE G. MANALANGPas encore d'évaluation
- 01 Application (Permit To Construct)Document1 page01 Application (Permit To Construct)jherica baltazar100% (1)
- ABTC Assessment ToolDocument8 pagesABTC Assessment Toolyam kuanPas encore d'évaluation
- Ipcr-Samillano, John Vanne D. Samillano, Rmt-Maayon RhuDocument5 pagesIpcr-Samillano, John Vanne D. Samillano, Rmt-Maayon RhuEdgar DumagpiPas encore d'évaluation
- Draft Moa Pgin Rhu KonsultaDocument3 pagesDraft Moa Pgin Rhu Konsultadumalneghrh 2017Pas encore d'évaluation
- Grievance CommitteeDocument1 pageGrievance CommitteeLouise salesPas encore d'évaluation
- DOH Ambulance RequiredDocument17 pagesDOH Ambulance RequiredAnonymous 7CnrWpzZf1Pas encore d'évaluation
- Pangasinan Municipalities by District & IlhzDocument1 pagePangasinan Municipalities by District & IlhzEdgar Garcia100% (2)
- AO 2016-0032 QS of Medical PositionsDocument12 pagesAO 2016-0032 QS of Medical PositionsTotoDodongGus100% (10)
- Form 5 - Rapid Health Assessment (MCI)Document1 pageForm 5 - Rapid Health Assessment (MCI)DELIVERY ROOMPas encore d'évaluation
- FP Form1 V3.0 2016Document3 pagesFP Form1 V3.0 2016Lorenz Joey Ricarte100% (2)
- Blood Request Form (Adult)Document2 pagesBlood Request Form (Adult)peanutbutter oh80% (5)
- DOH Clinical Privileging of HCWDocument21 pagesDOH Clinical Privileging of HCWahamedsahibPas encore d'évaluation
- 2022-0293 Interim Guidelines On The Assessment of Medical Certification of Cause of Death (MCCOD) in Health FacilitiesDocument7 pages2022-0293 Interim Guidelines On The Assessment of Medical Certification of Cause of Death (MCCOD) in Health FacilitiesBea Magbanua100% (2)
- Application FormDocument2 pagesApplication FormJohn Aldous Trinidad100% (1)
- HOspital Personnel OrderDocument3 pagesHOspital Personnel OrderNicoleAbdonPas encore d'évaluation
- 1.0 Functionality of The Local Health BoardDocument3 pages1.0 Functionality of The Local Health BoardEivenn Panerio100% (2)
- Loi MbfhiDocument11 pagesLoi MbfhiAnsams Fats100% (2)
- Work Experience SheetDocument7 pagesWork Experience SheetJerlin BienePas encore d'évaluation
- Letter of ApplicationDocument1 pageLetter of ApplicationJohn Louie SolitarioPas encore d'évaluation
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuPas encore d'évaluation
- Draft Ordinance (Birthing Homes Regulation)Document8 pagesDraft Ordinance (Birthing Homes Regulation)Zimm BasubasPas encore d'évaluation
- Section H. Morbidity Diseases ReportDocument5 pagesSection H. Morbidity Diseases ReportSeriel TismoPas encore d'évaluation
- Zero Reporting TemplateDocument1 pageZero Reporting Templatelance tabinas100% (2)
- Annex B Konsulta ChecklistDocument8 pagesAnnex B Konsulta ChecklistFret Ramirez Coronia RNPas encore d'évaluation
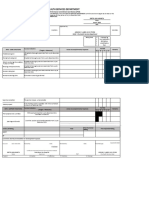
- City Health Services Department: Individual Performance Commitment and Review (IPCR)Document8 pagesCity Health Services Department: Individual Performance Commitment and Review (IPCR)Liecel Valdez100% (2)
- Accomplishment Report TemplateDocument6 pagesAccomplishment Report TemplateSample BakeshopPas encore d'évaluation
- F1 Plus Botika NG Bayan Manual of ProceduresDocument33 pagesF1 Plus Botika NG Bayan Manual of ProceduresArdenPas encore d'évaluation
- Tangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationDocument3 pagesTangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationbenPas encore d'évaluation
- Sponsorship LetterDocument5 pagesSponsorship LetterRosemarie Rimando CruzPas encore d'évaluation
- DOH ICT SytemDocument19 pagesDOH ICT Sytemricohizon99Pas encore d'évaluation
- Individual Performance Commitment and Review Form (Ipcrf) : Health and Nutrition ServicesDocument4 pagesIndividual Performance Commitment and Review Form (Ipcrf) : Health and Nutrition ServicesMonicahailey Macapobre0% (1)
- Salem Hospital Memo To StaffDocument6 pagesSalem Hospital Memo To StaffStatesman JournalPas encore d'évaluation
- 1 - Overview Training of The Revised MOP 6th Ed.Document14 pages1 - Overview Training of The Revised MOP 6th Ed.RHU Minalabac100% (1)
- Chief Nursing Officer: Thank You For Your Kind ConsiderationDocument1 pageChief Nursing Officer: Thank You For Your Kind ConsiderationLean Ashly Macarubbo100% (1)
- RA 9439 Anti Hospital DetentionDocument2 pagesRA 9439 Anti Hospital DetentionAling KinaiPas encore d'évaluation
- Presentation HEA OrientationDocument40 pagesPresentation HEA OrientationEdrheyl Limbaga BiadnesPas encore d'évaluation
- Assessment Tool - Level 1 HospitalDocument46 pagesAssessment Tool - Level 1 HospitalAnne Gravador-Nepomuceno100% (1)
- EO Epidemiology and SurveillanceDocument3 pagesEO Epidemiology and SurveillanceJeffson100% (1)
- HEPODocument8 pagesHEPOjay jay100% (1)
- DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1Document2 pagesDOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1jheanniver nablo100% (1)
- Revised Application Form DOH-HFSRB-QOP-01 Form1Document3 pagesRevised Application Form DOH-HFSRB-QOP-01 Form1Carol CasihanPas encore d'évaluation
- Application Form 2019Document5 pagesApplication Form 2019Rocky MontañerPas encore d'évaluation
- Tie Up Hema AnalyzerDocument4 pagesTie Up Hema AnalyzerKarina SantosPas encore d'évaluation
- Intro To Socio AnthroDocument75 pagesIntro To Socio AnthroKarina SantosPas encore d'évaluation
- RA MEDTECH MANILA Mar2019 PDFDocument94 pagesRA MEDTECH MANILA Mar2019 PDFKarina SantosPas encore d'évaluation
- Format For MLR 31.1.2012 PDFDocument2 pagesFormat For MLR 31.1.2012 PDFSurender SinghPas encore d'évaluation
- Communication Gaps in Nursing PDFDocument6 pagesCommunication Gaps in Nursing PDFAnonymous vUl83IptiSPas encore d'évaluation
- Mental Health History in U.S.Document3 pagesMental Health History in U.S.lazylawatudentPas encore d'évaluation
- Appropriate of Hospital Market: Measures AreasDocument21 pagesAppropriate of Hospital Market: Measures AreasMartin GoldPas encore d'évaluation
- FDAR Charting Sample: Date and Time Focus Data, Action, Response 12/30/14 8:00pm Post-OperativeDocument3 pagesFDAR Charting Sample: Date and Time Focus Data, Action, Response 12/30/14 8:00pm Post-OperativeNeojoy Zero-twoPas encore d'évaluation
- Basic Surgical Skills and Techniques From Jaypee Brothers Medical PubDocument6 pagesBasic Surgical Skills and Techniques From Jaypee Brothers Medical PubIshfaq AhPas encore d'évaluation
- 2.1 System Analysis 2.2 Identification 2.3 Preliminary Investigation 2.4 Feasibility StudyDocument66 pages2.1 System Analysis 2.2 Identification 2.3 Preliminary Investigation 2.4 Feasibility Studyjasmina0% (1)
- Aegys Pro-MRI: MRI Safety-Four Zones For Dummies PDFDocument3 pagesAegys Pro-MRI: MRI Safety-Four Zones For Dummies PDFaegysabetterwayPas encore d'évaluation
- Professional Services, Inc. V Ca G.R. 126297 Feb 2, 2010 PDFDocument10 pagesProfessional Services, Inc. V Ca G.R. 126297 Feb 2, 2010 PDFLloyd PerezPas encore d'évaluation
- LCM Summer Training Project Industrial Relations in BSPDocument35 pagesLCM Summer Training Project Industrial Relations in BSPRavi NegiPas encore d'évaluation
- Task Shifting & HRH Crisis: Field Experience and Current Thinking Within MSFDocument22 pagesTask Shifting & HRH Crisis: Field Experience and Current Thinking Within MSFBheru LalPas encore d'évaluation
- Casumpang V. Cortejo G.R. No. 171127 - March 11, 2015 FactsDocument1 pageCasumpang V. Cortejo G.R. No. 171127 - March 11, 2015 FactsjaymeebqPas encore d'évaluation
- Modul Bahasa Inggris KeperawatanDocument54 pagesModul Bahasa Inggris KeperawatanMaryPas encore d'évaluation
- Design Considerations For Hospitals and HotelsDocument18 pagesDesign Considerations For Hospitals and HotelsSaaviPas encore d'évaluation
- List of Hospitals 2Document10 pagesList of Hospitals 2Sirhc CeliotePas encore d'évaluation
- Sláintecare Action Plan 2023: Right Care Right Place Right TimeDocument41 pagesSláintecare Action Plan 2023: Right Care Right Place Right Timemary o'loughlinPas encore d'évaluation
- Vertigo Sympton ScaleDocument9 pagesVertigo Sympton ScaleIvan HoPas encore d'évaluation
- Understanding Liver BiopsyDocument4 pagesUnderstanding Liver BiopsyManisha ShakyaPas encore d'évaluation
- Firamita AhyarDocument2 pagesFiramita AhyarHennyartah HamzahPas encore d'évaluation
- Functional Endoscopic Sinus Surgery - Overview, Preparation, TechniqueDocument10 pagesFunctional Endoscopic Sinus Surgery - Overview, Preparation, TechniqueHendra SusantoPas encore d'évaluation
- Secrets To Effortless Spiritual Practice - Ebook by Supreme Master Ching HaiDocument103 pagesSecrets To Effortless Spiritual Practice - Ebook by Supreme Master Ching HaiThoai NguyenPas encore d'évaluation
- AdultDehydrationGuidelineJuly2015 PDFDocument3 pagesAdultDehydrationGuidelineJuly2015 PDFmarselamgePas encore d'évaluation
- Reviews of Educational MaterialDocument3 pagesReviews of Educational Materialshrutikathuria91Pas encore d'évaluation
- Analysis of The Implementation of Patient Guidance of Fall Risk at X HospitalDocument5 pagesAnalysis of The Implementation of Patient Guidance of Fall Risk at X HospitalyuniPas encore d'évaluation
- The Fundamentals of Critical Care Support Local ExDocument4 pagesThe Fundamentals of Critical Care Support Local ExStefanie KarinaPas encore d'évaluation
- Company ProfileDocument5 pagesCompany Profileganguly_ajayPas encore d'évaluation