Vous aimerez peut-être aussi
- A Loopy View of Telomere EvolutionDocument5 pagesA Loopy View of Telomere EvolutionLidya ZhuangPas encore d'évaluation
- Tr90 Flyer Eng (4 Pages)Document4 pagesTr90 Flyer Eng (4 Pages)Cherry San Diego0% (1)
- Outer Beauty Inner Balance: Acidic Vs Alkaline - PH Diet: by Christine HeathmanDocument22 pagesOuter Beauty Inner Balance: Acidic Vs Alkaline - PH Diet: by Christine HeathmanLidya ZhuangPas encore d'évaluation
- Brosur - Ageloc Youth enDocument20 pagesBrosur - Ageloc Youth enLidya ZhuangPas encore d'évaluation
- NaPCA Moisture Mist PIP EN PDFDocument2 pagesNaPCA Moisture Mist PIP EN PDFLidya ZhuangPas encore d'évaluation
- Drugs For Hypertension 2012Document13 pagesDrugs For Hypertension 2012Lidya ZhuangPas encore d'évaluation
- Chong-Physiatrist Powerpoint PDFDocument13 pagesChong-Physiatrist Powerpoint PDFLidya ZhuangPas encore d'évaluation
- EVDDocument2 pagesEVDLidya ZhuangPas encore d'évaluation
- Forensic AnalysisDocument21 pagesForensic AnalysisLidya ZhuangPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Prof Chase B. Wrenn - The True and The Good - A Strong Virtue Theory of The Value of Truth-Oxford University Press (2024)Document196 pagesProf Chase B. Wrenn - The True and The Good - A Strong Virtue Theory of The Value of Truth-Oxford University Press (2024)Mihaela DodiPas encore d'évaluation
- Lecture - 4 - 28june2023Document18 pagesLecture - 4 - 28june2023vanshikaPas encore d'évaluation
- Learning Objectives: Understanding The Self Module 1 - Sexual SelfDocument11 pagesLearning Objectives: Understanding The Self Module 1 - Sexual SelfMiss MegzzPas encore d'évaluation
- Marketing Plan For Optimo InternationalDocument47 pagesMarketing Plan For Optimo InternationalNiña Alfonso100% (1)
- Heat Transfer OperationsDocument10 pagesHeat Transfer OperationsShafique AhmedPas encore d'évaluation
- Cranial Deformity in The Pueblo AreaDocument3 pagesCranial Deformity in The Pueblo AreaSlavica JovanovicPas encore d'évaluation
- March 2009 Caro-Kann B12 by Sasa Velickovic Informant83Document6 pagesMarch 2009 Caro-Kann B12 by Sasa Velickovic Informant83kiprijanovPas encore d'évaluation
- Coursera Qs-Ans For Financial AidDocument2 pagesCoursera Qs-Ans For Financial AidMarno03Pas encore d'évaluation
- SCHEEL, Bernd - Egyptian Metalworking and ToolsDocument36 pagesSCHEEL, Bernd - Egyptian Metalworking and ToolsSamara Dyva86% (7)
- Business Finance Chapter 4Document15 pagesBusiness Finance Chapter 4chloe frostPas encore d'évaluation
- Food Safety Plan of Catalonia: GuidelinesDocument38 pagesFood Safety Plan of Catalonia: GuidelinesralapubsPas encore d'évaluation
- Dnyanadeep's IAS: UPSC Essay Series - 7Document2 pagesDnyanadeep's IAS: UPSC Essay Series - 7Rahul SinghPas encore d'évaluation
- "Article Critique" Walden University Methods For Evidence-Based Practice, Nursing 8200 January 28, 2019Document5 pages"Article Critique" Walden University Methods For Evidence-Based Practice, Nursing 8200 January 28, 2019Elonna AnnePas encore d'évaluation
- Mcqmate Com Topic 333 Fundamentals of Ethics Set 1Document34 pagesMcqmate Com Topic 333 Fundamentals of Ethics Set 1Veena DeviPas encore d'évaluation
- Antennas and Wave Propagation: Subject Code: Regulations: R16 JNTUH Class:III Year B.Tech ECE II SemesterDocument18 pagesAntennas and Wave Propagation: Subject Code: Regulations: R16 JNTUH Class:III Year B.Tech ECE II SemesterSriPas encore d'évaluation
- Alien Cicatrix II (Part 02 of 03) - The CloningDocument4 pagesAlien Cicatrix II (Part 02 of 03) - The CloningC.O.M.A research -stopalienabduction-Pas encore d'évaluation
- Constitutional Law Sem 5Document5 pagesConstitutional Law Sem 5Ichchhit SrivastavaPas encore d'évaluation
- Case KohortDocument37 pagesCase KohortNasir AhmadPas encore d'évaluation
- (Essential Histories) Waldemar Heckel - The Wars of Alexander The Great-Osprey PDFDocument97 pages(Essential Histories) Waldemar Heckel - The Wars of Alexander The Great-Osprey PDFJorel Fex100% (3)
- Child Development Assessment Tools in Low-Income and Middle-Income CountriesDocument9 pagesChild Development Assessment Tools in Low-Income and Middle-Income Countriesalibaba1888Pas encore d'évaluation
- 1st Annual Charity Golf Tournament For ChloeDocument2 pages1st Annual Charity Golf Tournament For ChloeM.G. PerezPas encore d'évaluation
- Unit5 v1.0022101210Document52 pagesUnit5 v1.0022101210Lily KkPas encore d'évaluation
- Wulandari - Solihin (2016)Document8 pagesWulandari - Solihin (2016)kelvinprd9Pas encore d'évaluation
- Maria Da Piedade Ferreira - Embodied Emotions - Observations and Experiments in Architecture and Corporeality - Chapter 11Document21 pagesMaria Da Piedade Ferreira - Embodied Emotions - Observations and Experiments in Architecture and Corporeality - Chapter 11Maria Da Piedade FerreiraPas encore d'évaluation
- RBG - CRM BRD - Marketing - v4.1Document68 pagesRBG - CRM BRD - Marketing - v4.1Manvi Pareek100% (2)
- Selvanathan-7e 17Document92 pagesSelvanathan-7e 17Linh ChiPas encore d'évaluation
- Filters SlideDocument17 pagesFilters SlideEmmanuel OkoroPas encore d'évaluation
- Subiecte Engleza August 2018 - V1Document6 pagesSubiecte Engleza August 2018 - V1DenisPas encore d'évaluation
- ESSAYDocument1 pageESSAYJunalie GregorePas encore d'évaluation
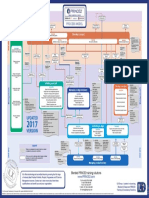
- p2 Process Model 2017Document1 pagep2 Process Model 2017Miguel Fernandes0% (1)