Vous aimerez peut-être aussi
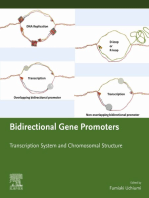
- Bidirectional Gene Promoters: Transcription system and chromosomal structureD'EverandBidirectional Gene Promoters: Transcription system and chromosomal structurePas encore d'évaluation
- Biotechnology and Drug Development for Targeting Human DiseasesD'EverandBiotechnology and Drug Development for Targeting Human DiseasesPas encore d'évaluation
- The Fruit Fly, Drosophila Melanogaster Modeling of Human Diseases (Part II)Document27 pagesThe Fruit Fly, Drosophila Melanogaster Modeling of Human Diseases (Part II)Amy SuarezPas encore d'évaluation
- Molecular Basis of Oxidative Stress: Chemistry, Mechanisms, and Disease PathogenesisD'EverandMolecular Basis of Oxidative Stress: Chemistry, Mechanisms, and Disease PathogenesisPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument31 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsfadimeatesPas encore d'évaluation
- Anastesi Lokal PDFDocument21 pagesAnastesi Lokal PDFshafarsoliPas encore d'évaluation
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument21 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherErlina WahyuPas encore d'évaluation
- Neuroblastoma The Clinical AspectsDocument21 pagesNeuroblastoma The Clinical AspectsErlina WahyuPas encore d'évaluation
- Insights to Neuroimmune BiologyD'EverandInsights to Neuroimmune BiologyIstvan BercziPas encore d'évaluation
- Cell and Tissue Destruction: Mechanisms, Protection, DisordersD'EverandCell and Tissue Destruction: Mechanisms, Protection, DisordersPas encore d'évaluation
- A Handbook of Mcqs in Toxicology: Muneeb U RehmanDocument53 pagesA Handbook of Mcqs in Toxicology: Muneeb U Rehmanquimicosorio100% (2)
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsJael AndreaPas encore d'évaluation
- NsaidDocument17 pagesNsaidnoviasinataPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument17 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsArya ChowdhuryPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument53 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistskaltrinaramaPas encore d'évaluation
- Mitochondrial Medicine: A Primer for Health Care Providers and Translational ResearchersD'EverandMitochondrial Medicine: A Primer for Health Care Providers and Translational ResearchersPas encore d'évaluation
- The Progress of Gut Microbiome Research Related To Brain DisordersDocument20 pagesThe Progress of Gut Microbiome Research Related To Brain DisordersVictoria HristovaPas encore d'évaluation
- Tumor Microenvironment Regulation of Tumor ExpansionD'EverandTumor Microenvironment Regulation of Tumor ExpansionPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument18 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsNurul HidayatiPas encore d'évaluation
- Cellular Response Mechanisms in Porphyromonas Gingivalis InfectionDocument25 pagesCellular Response Mechanisms in Porphyromonas Gingivalis Infectionwish to be fairyPas encore d'évaluation
- Crosstalk Between Anticancer Drugs and - 2021 - Current Research in PharmacologDocument9 pagesCrosstalk Between Anticancer Drugs and - 2021 - Current Research in PharmacologZac IngPas encore d'évaluation
- Green 2011Document5 pagesGreen 2011Arpan BhattacharyyaPas encore d'évaluation
- Your defenses against the coronavirus: A brief introduction to the immune systemD'EverandYour defenses against the coronavirus: A brief introduction to the immune systemPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument25 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsMadihaPas encore d'évaluation
- Spinal Interneurons: Plasticity after Spinal Cord InjuryD'EverandSpinal Interneurons: Plasticity after Spinal Cord InjuryLyandysha Viktorovna ZholudevaPas encore d'évaluation
- Epigenetics and MetabolomicsD'EverandEpigenetics and MetabolomicsPaban K. AgrawalaPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument35 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistshaloPas encore d'évaluation
- Fphys 14 1114231Document37 pagesFphys 14 1114231gguida0Pas encore d'évaluation
- Mitochondrial Dysfunction and Nanotherapeutics: Aging, Diseases, and Nanotechnology-Related Strategies in Mitochondrial MedicineD'EverandMitochondrial Dysfunction and Nanotherapeutics: Aging, Diseases, and Nanotechnology-Related Strategies in Mitochondrial MedicineMarcos Roberto de OliveiraPas encore d'évaluation
- Autophagy Dysfunction in Alzheimer's Disease and DementiaD'EverandAutophagy Dysfunction in Alzheimer's Disease and DementiaTadanori HamanoPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument15 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsArya ChowdhuryPas encore d'évaluation
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument31 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherAde Dian KaruniaPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument23 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsGina CubillasPas encore d'évaluation
- Antiaging DossierDocument27 pagesAntiaging DossiersattwaPas encore d'évaluation
- Arousal in Neurological and Psychiatric DiseasesD'EverandArousal in Neurological and Psychiatric DiseasesÉvaluation : 3 sur 5 étoiles3/5 (1)
- Immunology in the Twentieth Century: From Basic Science to Clinical ApplicationD'EverandImmunology in the Twentieth Century: From Basic Science to Clinical ApplicationPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument24 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsEcaterina Borovic-PavlovschiPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsTony AndersonPas encore d'évaluation
- Amphioxus Immunity: Tracing the Origins of Human ImmunityD'EverandAmphioxus Immunity: Tracing the Origins of Human ImmunityAn-Long XuPas encore d'évaluation
- Chemistry and Toxicology of Major Bioactive Substances in Inocybe MushroomsDocument13 pagesChemistry and Toxicology of Major Bioactive Substances in Inocybe MushroomsJosué DuartePas encore d'évaluation
- BiomoleculesDocument35 pagesBiomoleculesAna Paula Oliveira - NutricionistaPas encore d'évaluation
- Rahman and Rahman 2018 LancetDocument15 pagesRahman and Rahman 2018 LancetJoyeeta RahmanPas encore d'évaluation
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument37 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherColor BlackPas encore d'évaluation
- Food Poisoning Caused by Bacteria (Food Toxins) - IntechOpenDocument28 pagesFood Poisoning Caused by Bacteria (Food Toxins) - IntechOpenRubina KhatunPas encore d'évaluation
- Gene-Environment Interactions in Psychiatry: Nature, Nurture, NeuroscienceD'EverandGene-Environment Interactions in Psychiatry: Nature, Nurture, NeurosciencePas encore d'évaluation
- Common Tongue DisorderDocument9 pagesCommon Tongue DisorderEdo LiawandiPas encore d'évaluation
- First Page PDFDocument1 pageFirst Page PDFEdo LiawandiPas encore d'évaluation
- Who Consolidated Guidelines On TuberculosisDocument164 pagesWho Consolidated Guidelines On TuberculosisEdo LiawandiPas encore d'évaluation
- Journal Ppat 1007353Document7 pagesJournal Ppat 1007353Edo LiawandiPas encore d'évaluation
- GINA 2019 Main Report June 2019 Wms PDFDocument201 pagesGINA 2019 Main Report June 2019 Wms PDFAndrada PredaPas encore d'évaluation
- Asterixis PDFDocument3 pagesAsterixis PDFEdo LiawandiPas encore d'évaluation
- Nej Mic M 1814117Document1 pageNej Mic M 1814117Edo LiawandiPas encore d'évaluation
- 17 VitaminsCandEtreatmentDocument9 pages17 VitaminsCandEtreatmentEdo LiawandiPas encore d'évaluation
- Eighth Joint National Committee JNC-8 Guidelines ADocument8 pagesEighth Joint National Committee JNC-8 Guidelines AEdo LiawandiPas encore d'évaluation
- Effect of PH On The Activity of Potato CatalaseDocument1 pageEffect of PH On The Activity of Potato CatalaseNathuAndrews50% (2)
- The Pathophysiology of AtherosclerosisDocument15 pagesThe Pathophysiology of Atherosclerosisviper121Pas encore d'évaluation
- Gen Bio 1 Love of Lab Group Performance Task 1Document2 pagesGen Bio 1 Love of Lab Group Performance Task 1Ryan GañaPas encore d'évaluation
- Histology I: Dr. Mustafa Ghanim & Dr. Fatina HanbaliDocument35 pagesHistology I: Dr. Mustafa Ghanim & Dr. Fatina Hanbalijude dwekatPas encore d'évaluation
- MainDocument13 pagesMainIkmah FauzanPas encore d'évaluation
- Onion Cell Plasmolysis Lab Version 1Document4 pagesOnion Cell Plasmolysis Lab Version 1luckyduck28690% (1)
- Cells Test #1 Study Guide: Your Test Is: A Day: Tuesday 9/14, B Day: Wednesday 9/15Document2 pagesCells Test #1 Study Guide: Your Test Is: A Day: Tuesday 9/14, B Day: Wednesday 9/15Umar SulemanPas encore d'évaluation
- Instructions: Grade 10 Life Sciences November Paper 2Document14 pagesInstructions: Grade 10 Life Sciences November Paper 2JustinCase1991Pas encore d'évaluation
- Neuro HistologyDocument52 pagesNeuro HistologyZhiev Owen SullivanPas encore d'évaluation
- Case Study 1-BwilliamsDocument3 pagesCase Study 1-Bwilliamsapi-336564677Pas encore d'évaluation
- Blood TestDocument2 pagesBlood TestDhruv JainPas encore d'évaluation
- Functional Anatomy of Prokaryotic and Eukaryotic CellsDocument70 pagesFunctional Anatomy of Prokaryotic and Eukaryotic CellsTrixie De GuzmanPas encore d'évaluation
- MSC Genetics SyllabusDocument36 pagesMSC Genetics SyllabusMohak SahuPas encore d'évaluation
- Chapter 03 - Cell Structure and FunctionDocument32 pagesChapter 03 - Cell Structure and FunctionKhadija PrescottPas encore d'évaluation
- Cytoskeleton and Intracellular Communication Reviewer ORIGKEYDocument3 pagesCytoskeleton and Intracellular Communication Reviewer ORIGKEYnine nanoPas encore d'évaluation
- Mitosis WorksheetDocument4 pagesMitosis WorksheetAmna Jamshed67% (3)
- Chapter 2 NeuronDocument49 pagesChapter 2 NeuronNithinPas encore d'évaluation
- USMLE Step 1 First Aid 2020 30th - MICROBIOLOGYDocument82 pagesUSMLE Step 1 First Aid 2020 30th - MICROBIOLOGYArt PuffPas encore d'évaluation
- BiochemistryDocument12 pagesBiochemistryKitkat CasacopPas encore d'évaluation
- FRRRRRRRRRRRRRRRRRRRRRRRRRDocument11 pagesFRRRRRRRRRRRRRRRRRRRRRRRRRAnonymous Igsm89APas encore d'évaluation
- Hallmark of Cancer: Nur MahmudahDocument40 pagesHallmark of Cancer: Nur MahmudahFahmi SuhandinataPas encore d'évaluation
- 13 - GluconeogenesisDocument23 pages13 - GluconeogenesischeckmatePas encore d'évaluation
- Isolation of Chloroplast and Its ActivityDocument6 pagesIsolation of Chloroplast and Its ActivityEsen Nur ÖzlükPas encore d'évaluation
- Neurobiophysics2009 PreprintDocument52 pagesNeurobiophysics2009 PreprintsmiglemPas encore d'évaluation
- Abstract BookDocument241 pagesAbstract BookMuhammad AsaduzzamanPas encore d'évaluation
- Cell SpecializationDocument21 pagesCell SpecializationMatt NupenPas encore d'évaluation
- 2017 - Cre-loxP-Mediated Recombination - General Principles and Experimental ConsiderationsDocument12 pages2017 - Cre-loxP-Mediated Recombination - General Principles and Experimental ConsiderationsLucas PaulaPas encore d'évaluation
- Ebook Campbell Biology in Focus 2Nd Edition Urry Test Bank Full Chapter PDFDocument43 pagesEbook Campbell Biology in Focus 2Nd Edition Urry Test Bank Full Chapter PDFtristandoyledtnpkozbgj100% (13)
- Lipids BiochemDocument15 pagesLipids BiochemChan TalPas encore d'évaluation
- Centrosome Is To: CellsDocument3 pagesCentrosome Is To: CellsMarc Niño Christopher OcampoPas encore d'évaluation