Vous aimerez peut-être aussi
- Casp RCT Checklist PDFDocument4 pagesCasp RCT Checklist PDFMaria TamarPas encore d'évaluation
- Infeksi Saluran KemihDocument35 pagesInfeksi Saluran KemihLestari Amelia AdmPas encore d'évaluation
- Nur 194 Sas 1Document2 pagesNur 194 Sas 1Orange Alvarez100% (1)
- Seminar HD-RSUD Sleman 2019Document36 pagesSeminar HD-RSUD Sleman 2019herkamaya100% (1)
- 6INVAGINASIDocument18 pages6INVAGINASIhazelelPas encore d'évaluation
- Abdominal Pain in Children - Dr. Hermanto SP - BaDocument41 pagesAbdominal Pain in Children - Dr. Hermanto SP - Bajimmy_junPas encore d'évaluation
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanPas encore d'évaluation
- Asma Management 08 - 09 - 07Document81 pagesAsma Management 08 - 09 - 07botolkecapPas encore d'évaluation
- Retinopati DiabetikDocument5 pagesRetinopati DiabetikMuhammad Afriadi HamdanPas encore d'évaluation
- Tugas MSCT Rhino 2 Scan Rikha FixDocument29 pagesTugas MSCT Rhino 2 Scan Rikha FixRikha LiemiyahPas encore d'évaluation
- Congenital Adrenal HyperplasiaDocument2 pagesCongenital Adrenal HyperplasiaesyPas encore d'évaluation
- TELAAH KRITIS JURNAL Kel 2 - RCTDocument20 pagesTELAAH KRITIS JURNAL Kel 2 - RCTNama ManaPas encore d'évaluation
- EmpyemaDocument17 pagesEmpyemadeo_gratias14Pas encore d'évaluation
- Clabsi DR - RonaldDocument19 pagesClabsi DR - RonaldsilviPas encore d'évaluation
- CASP Checklist: Case Control Study How To Use This Appraisal ToolDocument6 pagesCASP Checklist: Case Control Study How To Use This Appraisal Toolanon_770867052Pas encore d'évaluation
- Dosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDocument1 pageDosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDenny RamdhanPas encore d'évaluation
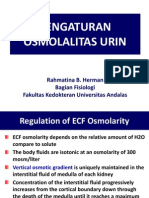
- Kuliah 3. Pengaturan Osmolalitas UrinDocument19 pagesKuliah 3. Pengaturan Osmolalitas UrinAnnisa DamayantiPas encore d'évaluation
- Burat-Buret Echo Romi Revised PDFDocument2 pagesBurat-Buret Echo Romi Revised PDFAsma.denmiPas encore d'évaluation
- Djenkolism ToxificationDocument5 pagesDjenkolism ToxificationSilvia RizkaPas encore d'évaluation
- Taping OA Genu Dr. SIsca Susantio, Sp. KFRDocument11 pagesTaping OA Genu Dr. SIsca Susantio, Sp. KFRDsk IndryPas encore d'évaluation
- Responsi Stemi Dr. Tuko SP - JP FixDocument56 pagesResponsi Stemi Dr. Tuko SP - JP FixcintaPas encore d'évaluation
- Tehnik - Tehnik Analgesia Post OperasiDocument32 pagesTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoPas encore d'évaluation
- Bi-Rads: (Breast Imaging-Reporting and Data System)Document30 pagesBi-Rads: (Breast Imaging-Reporting and Data System)Siti NirwanahPas encore d'évaluation
- PratikPatel - Duodenal AtresiaDocument1 pagePratikPatel - Duodenal AtresiaIkhlasia Amali MahzumPas encore d'évaluation
- Andhika Pangestu - Curicullum Vitae: 1. Personal InformationDocument6 pagesAndhika Pangestu - Curicullum Vitae: 1. Personal InformationPangestu DhikaPas encore d'évaluation
- Correlation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliDocument3 pagesCorrelation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliKarina NathaniaPas encore d'évaluation
- Hukum CourvoisierDocument1 pageHukum CourvoisierFahryHamkaPas encore d'évaluation
- Cataract 20surgery 2029 05 2008 131224024457 Phpapp01Document61 pagesCataract 20surgery 2029 05 2008 131224024457 Phpapp01Bboy ToonPas encore d'évaluation
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Osteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRDocument28 pagesOsteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRgita cahayaPas encore d'évaluation
- Chapter 65:: Psoriatic Arthritis and Reactive Arthritis:: Ana-Maria Orbai & John A. FlynnDocument12 pagesChapter 65:: Psoriatic Arthritis and Reactive Arthritis:: Ana-Maria Orbai & John A. FlynnDeb100% (1)
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Ophthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeDocument8 pagesOphthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeAdhe WagiPas encore d'évaluation
- Gir (Glucose Infussion Rate)Document9 pagesGir (Glucose Infussion Rate)arawindahaniastriPas encore d'évaluation
- Aldo Febriananto Kurniawan 22010112140205 Lap - Kti Bab ViiDocument19 pagesAldo Febriananto Kurniawan 22010112140205 Lap - Kti Bab ViiAfrilia ShafiraPas encore d'évaluation
- MataDocument163 pagesMataadelPas encore d'évaluation
- BGA Acid Base Stepwise PradikDocument43 pagesBGA Acid Base Stepwise PradikZulfadly NuralimPas encore d'évaluation
- Fetal Distress by DR Simon ByonanuweDocument23 pagesFetal Distress by DR Simon ByonanuweDr Simon ByonanuwePas encore d'évaluation
- Cholelithiasis: Shoofii Dzakiyyah Ulhaq Preceptor: Dr. Liza Nursanty, SP.B, M.Kes, FinacsDocument40 pagesCholelithiasis: Shoofii Dzakiyyah Ulhaq Preceptor: Dr. Liza Nursanty, SP.B, M.Kes, FinacsShofiDzakiyahUlhaqPas encore d'évaluation
- Syphilis CongenitalDocument5 pagesSyphilis CongenitalElisse StephaniePas encore d'évaluation
- Diagnosis & Tata Laksana Cad / CcsDocument40 pagesDiagnosis & Tata Laksana Cad / CcsIno HajrinPas encore d'évaluation
- Pityriasis Rosea - Background, Pathophysiology, EtiologyDocument4 pagesPityriasis Rosea - Background, Pathophysiology, EtiologysyahrulroziPas encore d'évaluation
- Operasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarDocument10 pagesOperasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarBlack Clover IdPas encore d'évaluation
- Blunt Adominal TraumaDocument13 pagesBlunt Adominal TraumaIlham RamadhanPas encore d'évaluation
- Pembahasan UKDI CLINIC 3 Batch Mei 2016Document662 pagesPembahasan UKDI CLINIC 3 Batch Mei 2016widi kusumaPas encore d'évaluation
- Jurnal Vivi HumairaDocument11 pagesJurnal Vivi HumairaMahyulPas encore d'évaluation
- PAD vs. DVTDocument3 pagesPAD vs. DVTKrystel BatinoPas encore d'évaluation
- Congestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCDocument25 pagesCongestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCYUSRIL ZUMADINSYAHPas encore d'évaluation
- K4. Diagnosis Holistik - EngDocument21 pagesK4. Diagnosis Holistik - EngBevila KorspoilvilPas encore d'évaluation
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 pagesKolestasis Intrahepatal Vs EkstrahepatalrikarikaPas encore d'évaluation
- Sarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalDocument2 pagesSarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalTan Chin AunPas encore d'évaluation
- Hipertensi JNC 8Document7 pagesHipertensi JNC 8Elisse StephaniePas encore d'évaluation
- BEDAH UMUM FKUI - Penatalaksanaan ApendisitisDocument7 pagesBEDAH UMUM FKUI - Penatalaksanaan ApendisitisRifda LatifaPas encore d'évaluation
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDocument17 pagesDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiFirda LestariPas encore d'évaluation
- Polycythemia Vera: Nurmaratu Thahirah Suaib C014172174Document12 pagesPolycythemia Vera: Nurmaratu Thahirah Suaib C014172174amiraPas encore d'évaluation
- Minggu I Miftahul Rauhan Bedah Plastik Ulkus DekubitusDocument25 pagesMinggu I Miftahul Rauhan Bedah Plastik Ulkus DekubitusmiftahulrauhanPas encore d'évaluation
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaD'EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaPas encore d'évaluation
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisD'EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- HyperthyroidismDocument14 pagesHyperthyroidismDian JuliantyPas encore d'évaluation
- Hypertiroid FixDocument11 pagesHypertiroid FixtiwiPas encore d'évaluation
- American Thyroid Association Guidelines For Detection of Thyroid DysfunctionDocument5 pagesAmerican Thyroid Association Guidelines For Detection of Thyroid DysfunctionUdsanee SukpimonphanPas encore d'évaluation
- CHED Scholarship Application FormDocument2 pagesCHED Scholarship Application FormMark DiamaPas encore d'évaluation
- Ellis 2023 HandoutsDocument26 pagesEllis 2023 HandoutsJalfePas encore d'évaluation
- Annmarie Villanueva ResumeDocument2 pagesAnnmarie Villanueva Resumeapi-496718295Pas encore d'évaluation
- Effective Team Work: Prepared & Presented By: Okanlomo Goke-OlatejuDocument21 pagesEffective Team Work: Prepared & Presented By: Okanlomo Goke-OlatejuOkanlomo Goke-OlatejuPas encore d'évaluation
- Challenges and Issues Faced Concerning ECEDocument4 pagesChallenges and Issues Faced Concerning ECEShiera GannabanPas encore d'évaluation
- Article Forum ELCDocument4 pagesArticle Forum ELCnurul izzatiPas encore d'évaluation
- Circ15 2012 PDFDocument7 pagesCirc15 2012 PDFJanice Villaroya Jarales-YusonPas encore d'évaluation
- Vertical Vs Horizontal Health Programs - Jan 13 - 2020Document13 pagesVertical Vs Horizontal Health Programs - Jan 13 - 2020KalkidanPhiliposPas encore d'évaluation
- Furosemide Drug ProfileDocument34 pagesFurosemide Drug ProfileNur Ilmi SofiahPas encore d'évaluation
- Policy DocDocument4 pagesPolicy DocRajatPas encore d'évaluation
- Restaurant Report Card - November 25, 2021Document6 pagesRestaurant Report Card - November 25, 2021KBTXPas encore d'évaluation
- Assignment For PFE701Document7 pagesAssignment For PFE701paku deyPas encore d'évaluation
- 68-Article Text-261-1-10-20191204Document9 pages68-Article Text-261-1-10-20191204Andi Dwi Resti JuliastutiPas encore d'évaluation
- 24 Brosur XN-1500 (SP-50, XN-20) + PLT-F + BF - PDocument2 pages24 Brosur XN-1500 (SP-50, XN-20) + PLT-F + BF - PVanda GoessPas encore d'évaluation
- The Concept of Necropolitics During The Pandemic of Covid-19 in BrazilDocument26 pagesThe Concept of Necropolitics During The Pandemic of Covid-19 in BrazilLaize RodriguesPas encore d'évaluation
- Case Report: Open Fracture 1/3 Distal Os Tibia and Fibula SinistraDocument34 pagesCase Report: Open Fracture 1/3 Distal Os Tibia and Fibula SinistraFarizka Dwinda HPas encore d'évaluation
- Fisiologia de La Cerda Ing. Magdiel SorianoDocument37 pagesFisiologia de La Cerda Ing. Magdiel SorianoFAUSTO JOSU� RODR�GUEZ AMADORPas encore d'évaluation
- g12 2nd Folk, Ballet, BallroomDocument82 pagesg12 2nd Folk, Ballet, BallroomJennifer ArnaizPas encore d'évaluation
- Jarrett, Liza ThesisDocument107 pagesJarrett, Liza ThesisAniko GyorgyPas encore d'évaluation
- Accomplishment February 2019Document8 pagesAccomplishment February 2019saphire donsolPas encore d'évaluation
- GRN777 Web PDFDocument125 pagesGRN777 Web PDFsuresh samineniPas encore d'évaluation
- Tety Yuliantine, Indasah, Sandu SiyotoDocument8 pagesTety Yuliantine, Indasah, Sandu SiyotopuriPas encore d'évaluation
- Water Is The Basic Necessity For The Functioning of All Life Forms That Exist On EarthDocument2 pagesWater Is The Basic Necessity For The Functioning of All Life Forms That Exist On EarthJust TinePas encore d'évaluation
- S - C R D: Ingle ASE Esearch EsignsDocument14 pagesS - C R D: Ingle ASE Esearch EsignsnugrahasakertabaratPas encore d'évaluation
- Physical Education Research Paper TopicsDocument8 pagesPhysical Education Research Paper Topicsefdvje8d100% (1)
- MPT Research ReportDocument7 pagesMPT Research ReportVenice De los ReyesPas encore d'évaluation
- IT Infrastructure in The Healthcare IndustryDocument7 pagesIT Infrastructure in The Healthcare IndustryHarsharaj MelantaPas encore d'évaluation
- CF Host Dept List 2023 24 v12Document111 pagesCF Host Dept List 2023 24 v12Antal Dorin CristianPas encore d'évaluation