Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Materials 09 01Document47 pagesMaterials 09 01Daniel Vergara ArcePas encore d'évaluation
- Monthly Plan For May 2016: MON TUE WED THU FRI Expected OutputsDocument1 pageMonthly Plan For May 2016: MON TUE WED THU FRI Expected OutputsDaniel Vergara ArcePas encore d'évaluation
- SLMCDocument5 pagesSLMCDaniel Vergara ArcePas encore d'évaluation
- Makati Medical CenterDocument2 pagesMakati Medical CenterDaniel Vergara ArcePas encore d'évaluation
- Risk Analysis: Risks Likeliho OD Impact ActionsDocument1 pageRisk Analysis: Risks Likeliho OD Impact ActionsDaniel Vergara ArcePas encore d'évaluation
- Name Gend Er Designation Organization Contact Number Signature (Day1) Signature (Day2)Document1 pageName Gend Er Designation Organization Contact Number Signature (Day1) Signature (Day2)Daniel Vergara ArcePas encore d'évaluation
- Barangay Council Orientation On Water, Sanitation and HygieneDocument2 pagesBarangay Council Orientation On Water, Sanitation and HygieneDaniel Vergara ArcePas encore d'évaluation
- RN Heal (Registered Nurses For Health Enhancement and Local Service)Document7 pagesRN Heal (Registered Nurses For Health Enhancement and Local Service)Daniel Vergara ArcePas encore d'évaluation
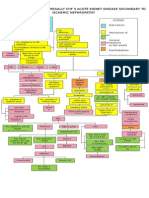
- Patho Aortic Stenosis ' (Colored)Document1 pagePatho Aortic Stenosis ' (Colored)Daniel Vergara ArcePas encore d'évaluation
- NCP - Excess Fluid Volume (Aortic Stenosis)Document3 pagesNCP - Excess Fluid Volume (Aortic Stenosis)Daniel Vergara Arce100% (3)
- Ncp-Ineffective Tissue Perfusion (Aortic Stenosis)Document2 pagesNcp-Ineffective Tissue Perfusion (Aortic Stenosis)Daniel Vergara Arce67% (3)
- Cues Nursing Diagnosis Scientific Rationale Objectives Nursing Intervention Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Scientific Rationale Objectives Nursing Intervention Rationale EvaluationDaniel Vergara ArcePas encore d'évaluation
- Herbal Medicines: How and When To Get The Herbal PlantsDocument10 pagesHerbal Medicines: How and When To Get The Herbal PlantsDaniel Vergara ArcePas encore d'évaluation
- Conflicts of InterestDocument27 pagesConflicts of InterestDaniel Vergara Arce100% (1)
- ChancroidDocument4 pagesChancroidDaniel Vergara ArcePas encore d'évaluation
- Nutrition in Cancer CareDocument7 pagesNutrition in Cancer CareDaniel Vergara ArcePas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Ethicon STEPS Advert 2020Document1 pageEthicon STEPS Advert 2020vlad910Pas encore d'évaluation
- Respiratory Sys QuestionsDocument2 pagesRespiratory Sys QuestionsShivangi BhandariPas encore d'évaluation
- Group 3 - Acute PancreatitisDocument5 pagesGroup 3 - Acute Pancreatitismelba040510Pas encore d'évaluation
- Hemifacial Spasm A NeurosurgicalDocument8 pagesHemifacial Spasm A NeurosurgicaldnazaryPas encore d'évaluation
- Grade 9: ScienceDocument19 pagesGrade 9: ScienceChristian ArcegaPas encore d'évaluation
- 13 - Daftar Pustaka NewDocument3 pages13 - Daftar Pustaka NewalfianiPas encore d'évaluation
- Renal TransplantationDocument33 pagesRenal TransplantationRohini Rai100% (1)
- ENT Batch 2022 Annual Paper-1Document9 pagesENT Batch 2022 Annual Paper-1mudassirahmedPas encore d'évaluation
- Ipmr AbbreviationsDocument2 pagesIpmr Abbreviationsapi-258242054Pas encore d'évaluation
- Y de RouxDocument5 pagesY de RouxFrancisco A. Villegas-LópezPas encore d'évaluation
- Nur 146 RleDocument47 pagesNur 146 RleKeziah Marie Chua Santa-AnaPas encore d'évaluation
- Module 2Document10 pagesModule 2Renee Andrei Concepcion MozarPas encore d'évaluation
- CPT 12 14 Hip System Long Stems Surgical TechniqueDocument22 pagesCPT 12 14 Hip System Long Stems Surgical TechniqueMery MerryPas encore d'évaluation
- Sedation Vacation in Neurocritical Care: A Proposal AlgorithmDocument3 pagesSedation Vacation in Neurocritical Care: A Proposal Algorithmrodolfo riosPas encore d'évaluation
- SurgeryDocument8 pagesSurgeryJessica RebbenPas encore d'évaluation
- PanoramikDocument38 pagesPanoramikStephanie Victoria100% (1)
- Visual Acuity and Intraocular Pressure After Cataract Extraction in Phacomorphic Angle Closure: A Retrospective ReviewDocument35 pagesVisual Acuity and Intraocular Pressure After Cataract Extraction in Phacomorphic Angle Closure: A Retrospective ReviewSandy AñoverPas encore d'évaluation
- Krok 2 - 2021 - 26 JulyDocument19 pagesKrok 2 - 2021 - 26 JulyNicole VinnikPas encore d'évaluation
- Introduction To NeuroanatomyDocument20 pagesIntroduction To NeuroanatomySurjagnee SannyamatPas encore d'évaluation
- J Jcin 2023 11 040Document19 pagesJ Jcin 2023 11 040GdfgdFdfdfPas encore d'évaluation
- NICU Booklet April2020Document90 pagesNICU Booklet April2020Popescu VioricaPas encore d'évaluation
- Get Through MRCOG Part 1 2nd EditionDocument142 pagesGet Through MRCOG Part 1 2nd Editionmustafa benmuhsen50% (2)
- Temporomandibular Joint DisordersDocument354 pagesTemporomandibular Joint Disordersz6f9cw8vwvPas encore d'évaluation
- The Study of Operation Theatre Utilization Amri Hospital BhubaneswarDocument46 pagesThe Study of Operation Theatre Utilization Amri Hospital BhubaneswarRakesh Kumar AcharjyaPas encore d'évaluation
- Varicose Veins Treatment by VSLSDocument10 pagesVaricose Veins Treatment by VSLSravuljindalPas encore d'évaluation
- Value of Bronchoscopy and Thoracoscopy in Respiratory MedicineDocument36 pagesValue of Bronchoscopy and Thoracoscopy in Respiratory MedicineMokwe Xavier CharlesPas encore d'évaluation
- 2010 Miniscrew Assisted Nonsurgical PalatalDocument10 pages2010 Miniscrew Assisted Nonsurgical PalatalMariana SantosPas encore d'évaluation
- BIRADSDocument94 pagesBIRADSSergio MoralesPas encore d'évaluation
- Neck TrianglesDocument6 pagesNeck TrianglesJay-arh SebusaPas encore d'évaluation
- Wesleyan University - Philippines: Immediate Newborn Cord Care CasesDocument5 pagesWesleyan University - Philippines: Immediate Newborn Cord Care CasesKristine CastilloPas encore d'évaluation