Académique Documents
Professionnel Documents
Culture Documents
Ajr 177 2 1770431
Transféré par
lilinTitre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Ajr 177 2 1770431
Transféré par
lilinDroits d'auteur :
Formats disponibles
Downloaded from www.ajronline.org by 180.246.59.76 on 11/22/17 from IP address 180.246.59.76. Copyright ARRS.
For personal use only; all rights reserved
CT of Small-Bowel Obstruction in
Children: Sensitivity and Specificity
Amal A. Jabra 1 OBJECTIVE. The aim of this study was to determine the sensitivity, specificity, and accu-
John Eng 2 racy of CT in the diagnosis of small-bowel obstruction in children.
Christopher G. Zaleski 3 MATERIALS AND METHODS. The CT scans of 30 children with surgically proven
George E. Abdenour, Jr.1 small-bowel obstruction, 22 children with ileus, and 29 children who served as controls were ret-
rospectively reviewed by two of four interpreters who were unaware of the children’s final diag-
Hao V. Vuong4
noses. Causes of obstruction in the patients included 19 adhesions, six cases of volvulus, five
Uwa O. Aideyan 1
intussusceptions, four strictures, and two cases each of internal hernia and abscess. Eight obstruc-
Elliot K. Fishman 2 tions had multiple causes. The CT scans were evaluated for the presence of small-bowel obstruc-
tion using a scale with five degrees of confidence. In cases of discrepancy of more than one level
of certainty, a third interpreter was consulted. Criteria for small-bowel obstruction included a dis-
crepancy in caliber between the proximal dilated and the more distal small bowels or generalized
small-bowel dilatation (>2.5 cm) in the presence of a collapsed colon. An interpreter’s rating that
an obstruction was either present or probable was considered a positive finding; a rating indicat-
ing that the interpreter was not sure whether an obstruction was present or believed that an ob-
struction was not probable or saw normal anatomic structures was considered a negative finding
for small-bowel obstruction. The cause and level of obstruction also were recorded.
RESULTS. There were 26 true-positive (87%) and four false-negative (13%) interpretations
for small-bowel obstruction. Among the interpretations of scans of patients with ileus, 68% were
true-negative and 32% were false-positive interpretations for small-bowel obstruction. Among
the control group, there were no false-positive readings. Sensitivity of CT was 87%, specificity
was 86%, and accuracy was 86%. In the scans of children 2 years and younger, CT had a sensitiv-
ity of 100% and specificity of 0%. Of the patients with surgically confirmed levels of obstruction,
the correct level of obstruction was described by both interpreters in 12 (86%) of 14 scans. The
causes of obstruction were correctly identified in 14 (47%) of 30 scans.
CONCLUSION. CT is both sensitive and specific for use in diagnosing small-bowel ob-
struction in children, especially in children older than 2 years.
Received September 20, 2000; accepted after revision
February 7, 2001.
T he diagnosis of small-bowel ob-
struction in children is usually
based on the clinical findings, ra-
diographs, or barium examinations. The use of
a control group to determine the sensitivity,
specificity, and accuracy of CT as an aid in di-
agnosing small-bowel obstruction in children.
1
Department of Radiology, University of Miami School of
Medicine, Jackson Memorial Medical Center, West Wing CT in the diagnosis of small-bowel obstruction Materials and Methods
279, 1611 N.W. 12th Ave., Miami, FL 33136. Address in children has been previously addressed, and The study population consisted of 30 consecutive
correspondence to A. A. Jabra. CT has been proposed as a useful adjunct diag- children with surgically proven small-bowel obstruc-
2 tion who had undergone abdominal CT scans for a va-
Department of Radiology, The Johns Hopkins Medical nostic procedure in detecting the presence of
Institutions, 600 N. Wolfe St., Baltimore, MD 21287. riety of clinical indications during their preoperative
small-bowel obstruction, its level, and its cause
3
Nemours Children’s Clinic, 807 Nira St., P. O. Box 5720, evaluation. Children with duodenal or neonatal ob-
[1]. Numerous publications have addressed the
Jacksonville, FL 32247. struction were excluded. Twenty-two consecutive
sensitivity, specificity, and accuracy of CT in the
4
Department of Radiology, Baptist Hospital, children who had been given a discharge diagnosis of
diagnosis of small-bowel obstruction in adults ileus and who had undergone abdominal CT as part of
8900 N. Kendall Dr., Miami, FL 33176.
[2–7]. No similar studies are available in pediat- their medical workup were also included. The control
AJR 2001;177:431–436
ric patients. In this study, we retrospectively re- group included 29 consecutive children who had un-
0361–803X/01/1772–431 viewed the CT findings in a series of children dergone abdominal CT for reasons unrelated to the
© American Roentgen Ray Society with either small-bowel obstruction or ileus and gastrointestinal tract—examination for possible me-
AJR:177, August 2001 431
Jabra et al.
tastasis from previous malignancies or for trauma IV contrast medium, and 28 children in the control children younger than 1 year, the presence of a dilated
workup. Their medical records indicated no gas- group also received oral contrast medium. Thirteen of small bowel was subjectively determined by the inter-
trointestinal pathology. The average age of the chil- 22 scans in the ileus group received IV contrast me- preters. A rating of “obstruction present” or “obstruc-
dren in the small-bowel obstruction group was 8.4 dium, and 18 received oral contrast medium. Of the tion probable” was considered a positive finding for
years; the average age of those in the ileus group was 30 patients with obstruction, 15 had IV contrast me- small-bowel obstruction. A rating of “not sure,” “not
10.2 years and of those in the control group, 9.6 years. dium, and 24 received oral contrast medium. probable,” or “normal study” was considered a negative
The causes of obstruction included 19 patients with The CT scans of all 81 children were random- finding for small-bowel obstruction. The interpreters
Downloaded from www.ajronline.org by 180.246.59.76 on 11/22/17 from IP address 180.246.59.76. Copyright ARRS. For personal use only; all rights reserved
adhesions, six with volvulus, five with intussuscep- ized, and each scan was retrospectively and indepen- were asked to identify the cause of obstruction. If no
tions, four with strictures, and two patients each with dently reviewed by a random combination of two of cause of obstruction was identified, a diagnosis of ad-
internal hernias and abscesses. Eight children had four interpreters. The interpreters were unaware of hesions was inferred. The interpreters were also asked
more than one cause for the obstruction. any patient’s final diagnosis. The scans were evalu- to determine the level of small-bowel obstruction—
The five of the CT scans were performed on a ated for the presence or absence of obstruction on a proximal (jejunal) or distal (distal jejunal or ileal).
9800 HiSpeed Advantage scanner (General Electric scale with five degrees of confidence—obstruction The interpreters’ diagnostic confidence ratings
Medical Systems, Milwaukee, WI), three were per- present, obstruction probable, not sure, obstruction were used to calculate receiver operating characteris-
formed on a Somaton DR3 scanner (Siemens, Erlan- not probable, and normal study. In the case of a dis- tic (ROC) curves for the detection of small-bowel ob-
gen, Germany), and two scans were performed on the crepancy of more than one level of certainty between struction. The ROCFIT program [8] was used to fit
DRH Siemens scanner. The remaining 71 scans were the two initial interpreters, a third interpreter was ROC curves to the confidence rating data.
performed on the DRH+ Siemens scanner. Scan pa- consulted so that a consensus could be reached. Proportions were compared using the Fisher’s ex-
rameters included 140–280 mA, 120–125 kVp, and The criteria used for diagnosing a small-bowel ob- act test as calculated by a software program (Stata,
0.7–3.0 sec of scanning time. Of the 81 scans per- struction have been previously described and include a version 6.0; Stata, College Station, TX). A p value of
formed, 39 of the scans were helical. Collimation was discrepancy in caliber between the dilated proximal less than 0.05 was considered statistically significant.
5–8 mm with data obtained at 5- to 10-mm intervals. and the more distal small bowels [1–3] (Fig. 1) or the
Both the usage and type of contrast medium var- presence of a dilated small bowel with a collapsed co-
ied, with some children receiving an oral contrast lon, particularly the ascending colon [1–3] (Fig. 2). A Results
agent; some, an IV contrast agent; some, both; and dilated small bowel was defined as one having a diame- Of the 30 children with small-bowel obstruc-
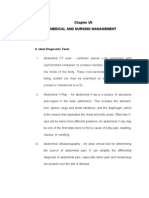
some, none. All 29 control scans were obtained using ter larger than 2.5 cm for children older than 1 year; for tion, there were 26 (87%) true-positive interpre-
tations for obstruction (Fig. 1) and four (13%)
false-negative interpretations (Table 1, Fig. 3).
There were no instances among the obstruction
group in which the interpreters were “not sure”
of their interpretations. There were no discrepant
interpretations requiring a third interpreter. In in-
terpreting the scans of children with ileus, 15
(68%) of 22 were true-negative findings (Fig. 4),
and seven (32%) of 22 were false-positive find-
ings for small-bowel obstruction. The former
group of 15 patients included two children
Fig.1.—8-month-old boy with small- whose scans elicited discrepancies in the evalua-
bowel obstruction resulting from ad- tions between the two initial interpreters. The
hesions. CT scan with IV contrast
medium shows difference in bowel third reviewer was not sure of the correct inter-
caliber with proximal dilated small pretation. These scans were considered to show
bowel (straight arrows) filled pre- negative findings for small-bowel obstruction.
dominantly with fluid and collapsed
distal small bowel (curved arrows).
Among the scans of the 29 controls, the review-
Ascites is present. ers had no false-positive interpretations nor did
they have any instances in which they were not
sure of their interpretations.The overall sensitiv-
ity of CT as an aid in diagnosing small-bowel
obstruction in this study was 87%, the specificity
was 86%, and the accuracy was 86%.
Summary of CT Scan
TABLE 1
Interpretations
Fig. 2.—17-year-old boy with small-
bowel obstruction. CT scan was Scans Scans
obtained 5 days after right nephrec- Interpreted Scans of
Revealing Revealing
tomy for trauma. Obstruction was for SBO Controls
SBO Ileus
produced by combination of adhe-
sions, segmental volvulus, and ileo- Positive 26 7 0
ilial intussusception related to
Meckle’s diverticulum. Scan shows Negative 4 15 29
intussusception (arrowheads). Also
Total 30 22 29
note small-bowel dilatation and col-
lapsed colon (arrows). Note.—SBO = small-bowel obstruction.
432 AJR:177, August 2001
CT of Small-Bowel Obstruction in Children
Downloaded from www.ajronline.org by 180.246.59.76 on 11/22/17 from IP address 180.246.59.76. Copyright ARRS. For personal use only; all rights reserved
Fig. 3.—12-year-old girl presenting with feeding intolerance and abdominal disten- Fig. 4.—16-year-old boy with ileus. CT scan shows generalized small-bowel dilata-
tion. Patient had undergone previous Nissen fundoplication and spinal instrumentation, tion (straight arrows) as well as dilatation of ascending colon (curved arrow).
which produced artifact. CT scan shows several localized mildly dilated air-filled
small-bowel loops resulting from compression and entrapment by adhesive bands.
Note typical hairpin appearance of bowel loop (arrows) frequently seen in closed-
loop obstruction. Diagnosis of obstruction was missed by both interpreters.
Sixteen of the 30 patients with small-bowel tional patient was diagnosed with a volvulus ers identified no cause for the obstruction in 16,
obstructions had the levels of obstruction de- involving most of the bowel. In this patient, including nine with isolated adhesions. The in-
scribed in the operative reports. Fourteen ob- both interpreters reported the level of obstruc- terpreters proposed likely causes for obstruction
structions were distal, and two were proximal. tion to be distal. in 10 of the patients, including two with multi-
In the 16 patients with surgically reported lev- Because the differentiation between ileus and ple causes. Of these, the interpreters correctly
els of obstruction, 14 were correctly diagnosed small-bowel obstruction is often the clinically identified three of five intussusceptions, one of
with obstructions by the interpreters, and two relevant question, a ROC curve for the detection three cases of volvulus, and one abscess. The in-
were given false-negative findings. Of the 14 of small-bowel obstruction (Fig. 5) was calcu- terpreters reported incorrect causes for the ob-
patients correctly diagnosed with obstructions, lated from a subset of the data (52 cases), which struction in the remaining five children. None of
the level of obstruction was correctly identified includes all patients except those in the control the four strictures were identified (one patient
by both interpreters in 12 (86%). The correct group. The area under the ROC curve was 0.84, had both a stricture and Crohn’s disease). Nei-
level of obstruction was identified by at least with a standard deviation of 0.06. ther of the two patients with an internal hernia
one interpreter in all 14 patients. One addi- Within the subset of 52 children, 10 chil- was identified. Of 19 patients with adhesions,
dren were 2 years or younger. In all these the findings on the scans of two were judged as
children, a small-bowel obstruction was de- false-negative for small-bowel obstruction.
tected on CT scans, although three had ileus Seven had both adhesions and other causes for
rather than an obstruction. Therefore, the the obstruction. Of the remaining 10 patients
specificity for the detection of small-bowel with isolated adhesions, the scan of one was
obstructions on the scans of these children misinterpreted as showing an intussusception;
was 0%, and the sensitivity was 100%. The nine patients were correctly diagnosed as hav-
remaining 42 children in the group with a ing a small-bowel obstruction with no apparent
disease were older than 2 years. For these cause for the obstruction. Thus, the scans of
children, the specificity of CT was 79% (15 these nine patients were correctly diagnosed by
of 19 patients) and the sensitivity was 83% inference as obstruction associated with adhe-
(19 of 23 patients). A comparison of the two sions. Overall, the interpreters identified the cor-
age groups shows a statistically significant rect cause for the obstruction in 14 (47%) of 30
difference in CT specificity (p = 0.02) but no scans, including intussusception (3/5), abscess
difference in CT sensitivity (p = 0.5). (1/2), volvulus (1/6), and adhesions (9/12 iso-
The scans for four of the 30 patients with ob- lated adhesions).
structions were judged as false–negative for ob-
struction. These included two patients with Discussion
Fig. 5.—Graph of fitted receiver operating characteris- adhesions, one with an internal hernia, and one CT is a well-established diagnostic proce-
tic curve for the detection of small-bowel obstruction
among the subset of abnormal cases. The area under with a volvulus around an omphalomesenteric dure for small-bowel obstruction evaluation
the curve is 0.84, with a standard deviation of 0.06. duct. In the remaining 26 patients, the interpret- in adults [2–14]. The use of CT in the diag-
AJR:177, August 2001 433
Jabra et al.
Downloaded from www.ajronline.org by 180.246.59.76 on 11/22/17 from IP address 180.246.59.76. Copyright ARRS. For personal use only; all rights reserved
Fig. 6.—8-month-old girl with prolonged abdominal distention. CT scan ob- Fig. 7.—Segmental small-bowel volvulus in 7-year-old girl. CT scan shows whirl sign
tained 23 days after exploratory laparatomy for unresectable neuroblastoma (arrows) produced by twisted mesenteric vessels.
shows area of ileoileal intussusception (arrows) causing obstruction, which
was missed by both interpreters. Note lack of fat density in intussusceptum.
nosis of small-bowel obstruction has not grade obstruction, and the higher range of values False-Negative Interpretations
been extensively addressed in the pediatric was reported in studies with a preponderance of One child with an internal hernia showed no
literature [1] with available papers generally patients with high-grade obstruction. The sensi- bowel dilatation on CT, likely because of an in-
representing case reports [15–17]. Although tivity of CT in studies with partial small-bowel termittent obstruction that was not present at the
CT is usually not the initial radiologic diag- obstruction ranged from 48–100% [4, 5]. time the scan was obtained. Another patient
nostic tool for small-bowel obstruction in In our study, we did not characterize the pa- showed a transition between mildly dilated
children, it can be used in some situations [1], tients as having low- versus high-grade ob- proximal and nondilated distal bowel. The distal
such as in those patients who have a long-stand- struction, a distinction that was generally not bowel wall was thickened, and an ileus related
ing obstruction with marked bowel distention made in the discharge diagnosis of or operative to inflammation rather than obstruction was
and for whom contrast studies may be unsuc- notes on the patients. The results of our study considered to be the cause. A third patient’s
cessful or too lengthy. CT can also be used in- fall within the range of results reported for scan showed air distention rather than increased
stead of a barium enema to diagnose distal adults in the literature. In our study, most of fluid content in the dilated loops. A bowel with
small-bowel obstruction if the enema is ex- the scans depicting ileus and small-bowel ob- a typical hairpin appearance of a closed-loop
pected to be very uncomfortable, such as in struction were not obtained on helical scan- obstruction (the bowel trapped by adhesions)
patients who have recently undergone sur- ners. The use of helical and multidetectors was missed (Fig. 3). Another patient’s scan
gery. CT is also a valuable tool for detecting scanners will likely yield technically better showed a borderline dilated distal small bowel
the extraluminal causes of bowel obstruction. scans and probably improved results. with mildly thickened walls. The ascending co-
Children with atypical clinical presentation In our study, we included a group of 22 pa- lon was filled with stool. This patient had a vol-
and unsuspected small-bowel obstruction tients with ileus because this diagnosis is likely vulus involving the last 60 cm of the ileum
may also first present for a CT study. the most difficult to differentiate from small- around an omphalomesenteric duct.
To our knowledge, the sensitivity of CT in re- bowel obstruction, both in clinical presentations
vealing small-bowel obstructions in children has and on radiographs. If the group with ileus is False-Positive Interpretations
not been previously reported, nor has the success excluded, the specificity of CT in revealing The CT scans of three children clearly met
of CT in determining the correct cause of ob- small-bowel obstruction increases to 100%. If the CT criteria for bowel obstruction. In these
struction been previously reported in a study in the control group is excluded and only the small- children, the interpreters considered the CT
which the reviewers were unaware of the final bowel obstruction and the ileus groups are in- scans as showing positive results for obstruc-
diagnosis. In our study, the sensitivity of CT in cluded, then the specificity of CT in revealing tion. These children improved with conservative
revealing small-bowel obstruction was deter- small-bowel obstruction decreases to 68%, and treatment, and their final discharge diagnosis
mined to be 87%, its specificity was 86%, and its the accuracy decreases to 79% (Fig. 5), values was ileus rather than obstruction. The readings
accuracy was 86%. In adult series, the sensitiv- that are still within the range reported in adult se- were therefore classified as false-positive. These
ity, specificity, and accuracy values were 63– ries. In our study, there were four false-negative patients raise a question about the nonsurgical
94%, 78–100%, and 65–95%, respectively [2–5]. and seven false-positive interpretations for diagnosis of small-bowel obstruction and the
The lower range of values was reported in stud- small-bowel obstruction, which affect the rates accuracy of the clinical diagnosis of ileus versus
ies with a preponderance of patients with low- of sensitivity and specificity, respectively. obstruction when symptoms improve without
434 AJR:177, August 2001
CT of Small-Bowel Obstruction in Children
surgical intervention. We know that obstruction nal mass, was suggested as the cause of obstruc- ropsoas location and was obvious when re-
caused by adhesions can improve or resolve tion by both interpreters in an 18-month-old viewed retrospectively. There was no bowel
with conservative treatment. In a study by Don- child with postoperative intussusception. The dilatation at the time of scanning, and the
ckier et al. [10], 28 (76%) of 37 patients thought second case of intussusception was missed in a scan was considered to show false-negative
to have simple (no strangulation) adhesive 5-month-old infant with ileoileal intussuscep- results for small-bowel obstruction. This pa-
small-bowel obstruction were successfully tion. The three cases in which the intussuscep- tient has been described in detail by Benson
Downloaded from www.ajronline.org by 180.246.59.76 on 11/22/17 from IP address 180.246.59.76. Copyright ARRS. For personal use only; all rights reserved
treated conservatively. In another study, 35% of tion was correctly identified were older children and Strauch [23].
patients with adhesions were treated conserva- (3, 17, and 18 years old). The difficulty in iden- When no cause for the obstruction is iden-
tively [18]. We believe that these three children tifying the two missed intussusceptions is likely tified at CT in a patient with a history of ab-
were true-positive for obstruction rather than a reflection of the younger age of the patients. dominal surgery, adhesions are usually
false-positive and that their obstructions im- The younger children are physically smaller, assumed to be the cause [2]. Of the 16 pa-
proved with conservative treatment. If these which could make the intussusception area less tients for whom our interpreters identified no
three patients are considered as among the true- obvious. Another reason for the difficulty with cause for obstruction, only nine (56%) had iso-
positive interpretations for obstruction, then the the diagnosis is the relative paucity of mesen- lated adhesions. Adhesions, however, were
specificity as well as the sensitivity in this study teric fat, which is usually identified between the correctly inferred as the diagnosis in nine
improves. The study population would then intussusceptum and the intussusception and is (75%) of 12 children with isolated adhesions.
consist of 33 children with obstruction, 19 with virtually diagnostic. In one series, 14 (88%) of In our study, the interpreters were not re-
ileus, and 29 controls. The sensitivity increases 16 adult intussusceptions showed this fatty area quested to determine whether closed-loop ob-
from 87% to 88%, and the specificity increases at CT [19]. In another adult study including CT struction or strangulation (ischemia) was
from 86% to 92%. scans and a small number of MR imaging stud- present. This area has received much attention
ies, 28 (68%) of 41 intussusceptions showed the in the recent adult literature [9, 11, 13, 14, 22,
Level of Obstruction fat on imaging [20]. No reports are available de- 24, 25]. Our interpreters did not identify the
The level of obstruction was correctly identi- scribing the frequency of visualizing fat within cause of obstruction in five patients with
fied by both interpreters in most children (86%) an intussusception on CT scans in children. The closed-loop obstructions (four with segmental
with levels of obstruction documented in the op- areas of intussusception in the two missed pa- volvulus and one with an entrapped ileal loop
erative records. CT is reported to be successful tients were obvious in retrospect but were by adhesions) (Fig. 3). To assess the accuracy
in determining the level of obstruction in up to smaller, with the fat density in the intussuscep- of CT in these diagnoses in children, a separate
97% of cases in adult series [5]. The level of ob- tion appearing on the scans more like the density study performed after familiarizing interpret-
struction was described in the operative records of water than that of fat (Fig. 6); no Hounsfield ers with the CT appearance of closed-loop ob-
for only 57% of our children and for most unit density measurements were obtained. This struction and strangulation obstruction may be
(88%) of these children, the level of obstruction finding is likely related to volume averaging of needed. In addition, standardizing the imaging
was described as distal. This distal location may the small amounts of fat with the adjacent soft technique in a prospective study would lead to
reflect the select nature of our small-bowel ob- tissues. In addition, the neuroblastoma may have more reliable results.
struction group; distal obstruction may be more satisfied search phenomenon, distracting from CT has a high sensitivity, specificity, and ac-
difficult to differentiate from ileus on conven- the correct diagnosis in the case of one child. curacy in revealing small-bowel obstructions
tional radiographs and could thus result in refer- The difficulty in diagnosing intussusception in in children, especially in children older than 2
ral to CT for the unexplained and indeterminate the young child may also explain the statisti- years. The level of obstruction was correctly
clinical and radiographic findings. cally significant lower specificity of differentiat- diagnosed in most patients. In this study, CT
ing small-bowel obstruction from ileus in had limited success in helping the interpreters
Cause of Obstruction children younger than 2 years old. to determine the cause of small-bowel obstruc-
In our study, the correct cause of obstruction Volvulus was detected correctly in only tion. Familiarity with the appearance of ob-
was identified in a limited number of patients. one of six patients and by only one inter- structive lesions on CT images and the use of
Five had specific causes, and nine were cor- preter. The scan of a second child with vol- helical and multidetector scanners will likely
rectly presumed to have adhesions (because no vulus showed a whirl pattern that was yield better results. A prospective study with a
cause for the obstruction was evident on the misinterpreted as an intussusception by both standardized imaging technique is needed for
CT scans). Considering all 30 cases with interpreters (Fig. 7). Familiarity with this more accurate results.
small-bowel obstruction (including four false- pattern in volvulus would improve the diag-
negative readings), the correct cause was therefore nostic accuracy [10, 17, 21]. In the remain-
made in only 47% of the patients. Excluding the ing four children, the volvulus did not have
false-negative readings, the correct cause of ob- either the whirl sign or a second pattern typi- References
struction was made in 14 (54%) of 26 children. cally seen as radial distribution of dilated 1. Jabra AA, Fishman EK. Small bowel obstruction
In adult series, the correct causes of obstruction bowel around engorged mesenteric vessels in the pediatric patient: CT evaluation. Abdom
have been reported as being detected in 76– converging towards the point of obstruction Imaging 1997;22:466–470
90% of cases [2, 3, 5, 7]. [9, 22]. One of these four children had an ad- 2. Megibow AJ, Balthazar EJ, Cho KC, Medwid SW,
Birnbaum BA, Noz ME. Bowel obstruction: evalu-
Diagnoses were missed for two of five pa- ditional ileoileal intussusception diagnosed
ation with CT. Radiology 1991;180:313–318
tients with intussusception in our study, though correctly by one of two interpreters. 3. Fukuya T, Hawes DR, Lu CC, Chang PJ, Barloon
the correct diagnosis of small-bowel obstruction Both internal hernias were missed. One of TJ. CT diagnosis of small-bowel obstruction: effi-
was made. Neuroblastoma, noted as an abdomi- two internal hernias was in an unusual ret- cacy in 60 patients. AJR 1992;158:765–769
AJR:177, August 2001 435
Jabra et al.
4. Maglinite DT, Gage SN, Harmon BH, et al. Ob- Bossart P. Detection of intestinal ischemia in pa- 18. Renzulli P, Krahenbuhl L, Sadowski C, Al-Adili F,
struction of the small intestine: accuracy and role tients with acute small-bowel obstruction due Maurer CA, Büchler MW. Moderne diagnostische Strat-
of CT in diagnosis. Radiology 1993;188:61–64 to adhesions or hernia: efficacy of CT. AJR egie beim Ileus. Zentralbl Chir 1998;123:1334–1339
5. Frager D, Medwid SW, Baer JW, Mollinelli B, 1996;166:67–71 19. Gayer G, Apter S, Hofmann C, et al. Intussuscep-
Friedman M. CT of small-bowel obstruction: 12. Maglinte DT, Balthazar EJ, Kelvin FM, Megibow tion in adults: CT diagnosis. Clin Radiol 1998;
value in establishing the diagnosis and determin- AJ. The role of radiology in the diagnosis of small- 53:53–57
ing the degree and cause. AJR 1994;162:37–41 bowel obstruction. AJR 1997;168:1171–1180 20. Warshauer DM, Lee JKT. Adult intussusception
Downloaded from www.ajronline.org by 180.246.59.76 on 11/22/17 from IP address 180.246.59.76. Copyright ARRS. For personal use only; all rights reserved
6. Frager DH, Baer JW, Rothpearl A, Bossart PA. 13. Balthazar EJ, Liebeskind ME, Macari M. Intesti- detected at CT or MR imaging: clinical-imaging
Distinction between postoperative ileus and me- nal ischemia in patients in whom small bowel ob- correlation. Radiology 1999;212:853–860
chanical small-bowel obstruction: value of CT struction is suspected: evaluation of accuracy, 21. Fisher JK. Computed tomographic diagnosis of
compared with clinical and other radiographic limitations, and clinical implications of CT in di- volvulus in intestinal malrotation. Radiology
findings. AJR 1995;164:891–894 agnosis. Radiology 1997;205:519–522 1981;140:145–146
7. Gazelle GS, Goldberg MA, Wittenberg J, Halpern 14. Ha HK, Kim JS, Lee MS, et al. Differentiation of 22. Balthazar EJ, Birnbaum BA, Megibow AJ, Gor-
EF, Pinkney L, Mueller PR. Efficacy of CT in distin- simple and strangulated small-bowel obstruc- don RB, Whelan CA, Hulnick DH. Closed-loop
guishing small-bowel obstruction from other causes tions: usefulness of known CT criteria. Radiology and strangulating intestinal obstruction: CT signs.
of small-bowel dilatation. AJR 1994; 162:43–478 1997;204:507–512 Radiology 1992;185:769–775
8. Metz CE. Some practical issues of experimental de- 15. Lerner A, Rossi TM, Hodge C, et al. A CT sign: 23. Benson JE, Strauch ED. Retropsoas hernia as a
sign and data analysis in radiological ROC studies. the “disappearing mass” as a clue to the diagnosis cause of chronic abdominal pain: CT diagnosis.
Invest Radiol 1989;24:234–245 of intermittent intestinal intussusception in chil- Pediatr Radiol 1998;28:312–314
9. Balthazar EJ. CT of small-bowel obstruction. dren. Comput Radiol 1984;8:387–390 24. Balthazar EJ, Bauman JS, Megibow AJ. CT diag-
AJR 1994;162:255–261 16. Mori H, Hayashi K, Futagawa S, et al. Vascular nosis of closed loop obstruction. J Comput Assist
10. Donckier V, Closset J, Gansbeke DV, et al. Con- compromise in chronic volvulus with midgut Tomogr 1985;9:953–955
tribution of computed tomography to decision malrotation. Pediatr Radiol 1987;17:277–281 25. Zalcman M, Gansbeke DV, Lalmand B, Braudé P,
making in the management of adhesive small 17. Yoon HK, Han BK. Chronic midgut volvulus Closset J, Struyven J. Delayed enhancement of the
bowel obstruction. Br J Surg 1998;85:1071–1074 with messenteric lymphangioma: a case report. bowel wall: a new CT sign of small bowel strangu-
11. Frager D, Baer JW, Medwid SW, Rothpearl A, Pediatr Radiol 1998;28:611 lation. J Comput Assist Tomogr 1996;20:379–381
436 AJR:177, August 2001
Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Case Study GI #4Document5 pagesCase Study GI #4Jenny JendersPas encore d'évaluation
- Treatment of Constipation in Older Adult AAFPDocument8 pagesTreatment of Constipation in Older Adult AAFPTom KirklandPas encore d'évaluation
- Typhoid FeverDocument24 pagesTyphoid FeverHazielle BondocPas encore d'évaluation
- Primary Biliary CholangitisDocument23 pagesPrimary Biliary CholangitisAbdul hadiPas encore d'évaluation
- Case study analyzes GI tract issuesDocument2 pagesCase study analyzes GI tract issuesSEBASTIEN ANDREI BUENAFEPas encore d'évaluation
- Colcistectomia FenestradaDocument8 pagesColcistectomia FenestradaLuis David AguileraPas encore d'évaluation
- Git MotilityDocument68 pagesGit MotilityGaurav SinghPas encore d'évaluation
- 11 Foods That Can Cause HeartburnDocument10 pages11 Foods That Can Cause HeartburnSelim HanPas encore d'évaluation
- Estimasi Biaya Bedah DigestifDocument2 pagesEstimasi Biaya Bedah DigestifDei RahayuPas encore d'évaluation
- 2020.08.24 - PPT Sidang UP - Roland Ma'arif Pangestu - 130110170020Document31 pages2020.08.24 - PPT Sidang UP - Roland Ma'arif Pangestu - 130110170020FIKRI MUHAMMADPas encore d'évaluation
- Digestive NutrientsDocument6 pagesDigestive NutrientsCXT EnterprisePas encore d'évaluation
- Typhoid Fever Case Study in a ChildDocument43 pagesTyphoid Fever Case Study in a ChildJef Sembrano DiplomaPas encore d'évaluation
- Anorectal Malformations: NM Rika Trismayanti SPB, Spba (K)Document14 pagesAnorectal Malformations: NM Rika Trismayanti SPB, Spba (K)niaPas encore d'évaluation
- Epidemiology and Pathophysiology of Diverticular Disease: August 2009Document7 pagesEpidemiology and Pathophysiology of Diverticular Disease: August 2009kuro hanabusaPas encore d'évaluation
- GI Bleeding PDFDocument9 pagesGI Bleeding PDFTia Amalia Puti RenaeryPas encore d'évaluation
- CP Intestinal Obstruction Chap7Document57 pagesCP Intestinal Obstruction Chap7Katherine 'Chingboo' Leonico LaudPas encore d'évaluation
- Congenital Anomalies of GiDocument94 pagesCongenital Anomalies of GiPadmaPas encore d'évaluation
- Acute Abdominal Pain GuideDocument19 pagesAcute Abdominal Pain GuideAudricPas encore d'évaluation
- Studi Penggunaan Oad Pada Pasien Diabetes Melitus Tipe 2Document13 pagesStudi Penggunaan Oad Pada Pasien Diabetes Melitus Tipe 2Fatwaa AizzahraaPas encore d'évaluation
- Nasogastric TubeDocument5 pagesNasogastric TubeangelaPas encore d'évaluation
- Chronic Diarrhea and Malabsorption GuideDocument50 pagesChronic Diarrhea and Malabsorption GuideIPNATC NEPAL100% (1)
- Final Grand Case-GeneralaoDocument110 pagesFinal Grand Case-GeneralaoLovely Hope LugatimanPas encore d'évaluation
- Malabsorption Seminar: Causes and Nursing CareDocument42 pagesMalabsorption Seminar: Causes and Nursing CaresomivipinPas encore d'évaluation
- Small Intestinal Bacterial Overgrowth - Management - UpToDate (2018)Document8 pagesSmall Intestinal Bacterial Overgrowth - Management - UpToDate (2018)Moileon2011Pas encore d'évaluation
- Intestinal Cleanse: SCIENCE (Continued)Document2 pagesIntestinal Cleanse: SCIENCE (Continued)finePas encore d'évaluation
- Gastroesophageal Reflux Disease (Gerd) & Hiatal Hernia: MedsurgicalDocument2 pagesGastroesophageal Reflux Disease (Gerd) & Hiatal Hernia: Medsurgical2A - Nicole Marrie HonradoPas encore d'évaluation
- Dismat 2 - Penyakit Hepar Dan Git - Althea Saarah Nafisah - 28072022 - AkaDocument65 pagesDismat 2 - Penyakit Hepar Dan Git - Althea Saarah Nafisah - 28072022 - AkaeaaaaPas encore d'évaluation
- Esophagitis: Causes, Symptoms and TreatmentDocument10 pagesEsophagitis: Causes, Symptoms and TreatmentRamya SriPas encore d'évaluation
- HePatic AbscessDocument67 pagesHePatic AbscessCharlie Mignonette BalaPas encore d'évaluation
- Chronic PancreatitisDocument94 pagesChronic PancreatitisDipendra PoudelPas encore d'évaluation