Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
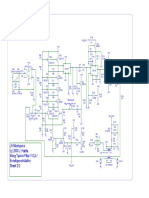
- JH Minotaurus Schematic p2 - Moog Taurus Filter VCA ENV EmulatorDocument1 pageJH Minotaurus Schematic p2 - Moog Taurus Filter VCA ENV EmulatorcrackintheshatPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Ladder Filter Design, Fabrication, & Measurement - EECS 142 Lab 3 Background ReadingDocument27 pagesLadder Filter Design, Fabrication, & Measurement - EECS 142 Lab 3 Background ReadingcrackintheshatPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- JH Minotaurus Schematic p1 - Moog Taurus Filter VCA ENV EmulatorDocument1 pageJH Minotaurus Schematic p1 - Moog Taurus Filter VCA ENV EmulatorcrackintheshatPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- MF 101Document14 pagesMF 101Kara JohnstonPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Transistor Matching - Ian Fritz - Transmat0011 - 144Document5 pagesTransistor Matching - Ian Fritz - Transmat0011 - 144crackintheshatPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Eviews F HerapeuticsDocument17 pagesEviews F HerapeuticscrackintheshatPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- SMR-4MKII Filter Analysis - Resonance Control Analysis On Page 9 - Oliviere From Mutable InstrumentsDocument10 pagesSMR-4MKII Filter Analysis - Resonance Control Analysis On Page 9 - Oliviere From Mutable InstrumentscrackintheshatPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Moog MF-101 LPF SchematicsDocument5 pagesMoog MF-101 LPF SchematicscrackintheshatPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- EHX Black Finger PDFDocument1 pageEHX Black Finger PDFГеоргий Ельцов100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- LVL - LOK-500 v1.13 SWITCH WIRINGDocument1 pageLVL - LOK-500 v1.13 SWITCH WIRINGcrackintheshatPas encore d'évaluation
- LVL - Lok-500 v1.13 SchematicDocument1 pageLVL - Lok-500 v1.13 SchematiccrackintheshatPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Russian FET CompressorDocument15 pagesRussian FET CompressorcrackintheshatPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- LVL - LOK-500 v1.13 BOMDocument1 pageLVL - LOK-500 v1.13 BOMcrackintheshatPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Buddha CompDocument1 pageBuddha CompcrackintheshatPas encore d'évaluation
- EnigmaDocument2 pagesEnigmaDwight JonesPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Outcome of A Histamine-Restricted Diet Based On Chart Audit - JANICE M. VICKERSTAFF JONEJA PHD RDNDocument15 pagesOutcome of A Histamine-Restricted Diet Based On Chart Audit - JANICE M. VICKERSTAFF JONEJA PHD RDNcrackintheshatPas encore d'évaluation
- Electronics Today Magazine - January 1985 (ETI)Document76 pagesElectronics Today Magazine - January 1985 (ETI)crackintheshat100% (1)
- EC445 Final - Paper1Document22 pagesEC445 Final - Paper1crackintheshatPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Basic Transformer Hook Up DataDocument2 pagesBasic Transformer Hook Up DatacrackintheshatPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Pirani Gauge JST - 20131220Document9 pagesPirani Gauge JST - 20131220crackintheshatPas encore d'évaluation
- Summary of Terrorist Attacks of September 11, 2001Document6 pagesSummary of Terrorist Attacks of September 11, 2001ShaktikumarPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Barriga de Trigo - William DavisDocument19 pagesBarriga de Trigo - William Davisfilipecosta1993Pas encore d'évaluation
- Histamine and Histamine Intolerance1 3 Laura Maintz and Natalija Novak Znu00507001185 PDFDocument12 pagesHistamine and Histamine Intolerance1 3 Laura Maintz and Natalija Novak Znu00507001185 PDFcrackintheshatPas encore d'évaluation
- Lab 4 - Push-Pull Biasing, Buck Converter, ECGDocument20 pagesLab 4 - Push-Pull Biasing, Buck Converter, ECGcrackintheshatPas encore d'évaluation
- Lab 07 - Op-AmpsDocument49 pagesLab 07 - Op-AmpscrackintheshatPas encore d'évaluation
- GP6 Users Manual enDocument61 pagesGP6 Users Manual enJosé Antonio TapiaPas encore d'évaluation
- Lab 08 - Op-Amp ApplicationsDocument60 pagesLab 08 - Op-Amp ApplicationscrackintheshatPas encore d'évaluation
- Lab 2 - Transistor BiasDocument12 pagesLab 2 - Transistor Biascrackintheshat100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Lab 05 - 3 Stage AmpliferDocument47 pagesLab 05 - 3 Stage AmplifercrackintheshatPas encore d'évaluation
- Lab 06 - Mosfet & JfetsDocument64 pagesLab 06 - Mosfet & JfetscrackintheshatPas encore d'évaluation
- Epigenetic ModificationsDocument1 pageEpigenetic ModificationsFerny PintoPas encore d'évaluation
- The Cell Cycle and Cell Division: I G N MayunDocument39 pagesThe Cell Cycle and Cell Division: I G N Mayunigus696Pas encore d'évaluation
- 12 Transgenic Animals - Prospect For Improving Livestock Productivity PDFDocument20 pages12 Transgenic Animals - Prospect For Improving Livestock Productivity PDFEloi AquinoPas encore d'évaluation
- Case Study 6Document2 pagesCase Study 6api-265054719Pas encore d'évaluation
- Isozyme, Ribozyme, AbzymeDocument3 pagesIsozyme, Ribozyme, Abzymeshazeen shoaibPas encore d'évaluation
- Protein Based NanostructuresDocument3 pagesProtein Based NanostructuresDannyMarlonJ100% (1)
- Metabolic Biochemistry: Title: Determination of Protein Concentration Using Biuret AssayDocument6 pagesMetabolic Biochemistry: Title: Determination of Protein Concentration Using Biuret AssayLeong Kok ZhengPas encore d'évaluation
- Dgge (Denaturing Gradient Gel Electrophoresis)Document4 pagesDgge (Denaturing Gradient Gel Electrophoresis)twangpanPas encore d'évaluation
- Chapter 16 - Origin and Evolution of Microbial Life - PPTX DimaporoDocument39 pagesChapter 16 - Origin and Evolution of Microbial Life - PPTX DimaporoRamon Chito S. PudelananPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Effect of Naringenin On Alcl3 Induced Alzheimir Disease in Drosophila FlyDocument27 pagesEffect of Naringenin On Alcl3 Induced Alzheimir Disease in Drosophila FlyPeter AiyedePas encore d'évaluation
- MTG Lifesci en 18 Sept 2014Document184 pagesMTG Lifesci en 18 Sept 2014api-202349222Pas encore d'évaluation
- Cellsummativereview AnswersDocument5 pagesCellsummativereview Answersapi-422802678Pas encore d'évaluation
- Biochem Module 2Document6 pagesBiochem Module 2Arvin CoirnePas encore d'évaluation
- B.I Sec 4.Document18 pagesB.I Sec 4.dark SpizroPas encore d'évaluation
- Teacher PlacementsDocument9 pagesTeacher Placementsapi-239505062Pas encore d'évaluation
- Biological OxidationDocument42 pagesBiological OxidationSapana Subedi100% (1)
- Full Download Test Bank Essential Biochemistry 3rd Edition Pratt Cornely PDF Full ChapterDocument36 pagesFull Download Test Bank Essential Biochemistry 3rd Edition Pratt Cornely PDF Full Chaptercassatemesoseme7m8v100% (18)
- Virtual Screening Tutorial Histamine H4 by C. de GraafDocument3 pagesVirtual Screening Tutorial Histamine H4 by C. de GraafPace RaditPas encore d'évaluation
- Grade 10 Daily Lesson PlanDocument3 pagesGrade 10 Daily Lesson PlanRod ReyesPas encore d'évaluation
- BIOLOGICAL OXIDATION & Principle of Energy MetabolismDocument84 pagesBIOLOGICAL OXIDATION & Principle of Energy MetabolismAnikusaSaniariPas encore d'évaluation
- How Genes WorkDocument47 pagesHow Genes WorkJelly Joy CampomayorPas encore d'évaluation
- Bio MoleculesDocument45 pagesBio MoleculesAngelica MartinPas encore d'évaluation
- 9 - Nonlinear PharmacokineticsDocument44 pages9 - Nonlinear PharmacokineticsYuppie RajPas encore d'évaluation
- Microbial Metabolism - EnzymesDocument14 pagesMicrobial Metabolism - EnzymesSaint TzyPas encore d'évaluation
- Biotechnology Products Fda PDFDocument36 pagesBiotechnology Products Fda PDFJosé Carlos Solís SuárezPas encore d'évaluation
- Chestionar Consultanta NutritieDocument8 pagesChestionar Consultanta NutritieRalucaPas encore d'évaluation
- Lab Report 5 Protein Solubility and PHDocument3 pagesLab Report 5 Protein Solubility and PHDan Floyd FernandezPas encore d'évaluation
- Typhoon 9210 Variable ImagerDocument4 pagesTyphoon 9210 Variable ImagerhalfanglePas encore d'évaluation
- Congratulations For Reaching The Last ModuleDocument12 pagesCongratulations For Reaching The Last ModuleRaphael Louis DacanayPas encore d'évaluation
- Chapter 2 HomeworkDocument5 pagesChapter 2 HomeworkKvn4N6Pas encore d'évaluation
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomD'EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyD'EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookD'EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainD'EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainÉvaluation : 3.5 sur 5 étoiles3.5/5 (38)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarD'EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarÉvaluation : 5 sur 5 étoiles5/5 (351)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonD'EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonÉvaluation : 3.5 sur 5 étoiles3.5/5 (33)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeD'EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifePas encore d'évaluation
- The Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoD'EverandThe Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoPas encore d'évaluation