Vous aimerez peut-être aussi
- Pneumonia: Neonates To AdolescentsDocument32 pagesPneumonia: Neonates To AdolescentsAthenaTudino100% (2)
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 pagesPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- Weekly Lesson Plans Spanish 1-2Document8 pagesWeekly Lesson Plans Spanish 1-2JaimePas encore d'évaluation
- Chomsky, N. (1980) - Binding PDFDocument47 pagesChomsky, N. (1980) - Binding PDFZhi ChenPas encore d'évaluation
- Pneumonia and BronchiolitisDocument48 pagesPneumonia and Bronchiolitisshashank panwarPas encore d'évaluation
- PneumoniaDocument66 pagesPneumoniaumanantini06100% (1)
- Pneumonia Seminar HKNDocument66 pagesPneumonia Seminar HKNMahendra Yogi SemaraPas encore d'évaluation
- Infectious Disorder: Prepared By: Dellero, Sarah Joy P. BSN3-DDocument19 pagesInfectious Disorder: Prepared By: Dellero, Sarah Joy P. BSN3-Dngoto88Pas encore d'évaluation
- Respiratory System For KidsDocument9 pagesRespiratory System For Kidssammim3418Pas encore d'évaluation
- Community Acquired Pneumonia: Villon, Faith Therese LDocument19 pagesCommunity Acquired Pneumonia: Villon, Faith Therese LPaul Gabriel CasquejoPas encore d'évaluation
- Approach To CoughDocument5 pagesApproach To CoughZulaikha HattaPas encore d'évaluation
- Acute Lower Respiratory InfectionsDocument28 pagesAcute Lower Respiratory InfectionsAs Minhas OrigensPas encore d'évaluation
- Acute Respiratory Infection: Darmawan B SetyantoDocument84 pagesAcute Respiratory Infection: Darmawan B SetyantonurhasanahPas encore d'évaluation
- Lower Rspiratory Tract - Pneumonia-: BalanceDocument7 pagesLower Rspiratory Tract - Pneumonia-: BalanceSofronio OmboyPas encore d'évaluation
- AsthmaDocument66 pagesAsthmaapi-3729824100% (4)
- Acute Respiratory InfectionsDocument145 pagesAcute Respiratory InfectionsManuel VIc O. Lacaya100% (1)
- PnemoniaDocument38 pagesPnemoniaArjumand AliPas encore d'évaluation
- Nursing CS CroupDocument1 pageNursing CS Croupreuben kadarajaPas encore d'évaluation
- Respirology Division, Department of Child Health, Udayana University Medical School/Sanglah Hospital, DenpasarDocument59 pagesRespirology Division, Department of Child Health, Udayana University Medical School/Sanglah Hospital, DenpasarWita FitriyaniPas encore d'évaluation
- Respiratory Disorders in ChildrenDocument77 pagesRespiratory Disorders in ChildrenJharaPas encore d'évaluation
- Pneumonia PresentationDocument23 pagesPneumonia Presentationapi-546694141Pas encore d'évaluation
- Wheezing in Children - ASIF KHUHRODocument22 pagesWheezing in Children - ASIF KHUHROShahnawazPas encore d'évaluation
- Before Learning: Tips For Active LearningDocument19 pagesBefore Learning: Tips For Active LearningSontoshMBsmmuPas encore d'évaluation
- 4e8ae48410.TERAPI ISPA DAN ISPBDocument56 pages4e8ae48410.TERAPI ISPA DAN ISPBAbd HarisPas encore d'évaluation
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaMaria Cristina100% (1)
- Acute CoughDocument14 pagesAcute CoughGeeza Gem VicencioPas encore d'évaluation
- W1 L3 Wheezy InfantsDocument36 pagesW1 L3 Wheezy InfantsAnas FikriPas encore d'évaluation
- Lower Respiratory Tract InfectionDocument9 pagesLower Respiratory Tract InfectionNamrah AfzalPas encore d'évaluation
- GS Bronchial Asthma Bronchiectasis EmphysemaDocument68 pagesGS Bronchial Asthma Bronchiectasis EmphysemaBibika MallaPas encore d'évaluation
- Respiratory Infections PDFDocument27 pagesRespiratory Infections PDFEmmanuel MachelelePas encore d'évaluation
- Respiratory PathophysDocument1 pageRespiratory PathophysTori IkeharaPas encore d'évaluation
- Roseola Infantum (Exanthem Subitum) Pathpophysiology: Infected Saliva by The HHV-6 VirusDocument7 pagesRoseola Infantum (Exanthem Subitum) Pathpophysiology: Infected Saliva by The HHV-6 VirusElle RosalesPas encore d'évaluation
- Persistent - Recurrent PneumoniaDocument35 pagesPersistent - Recurrent PneumoniaVishal SidanaPas encore d'évaluation
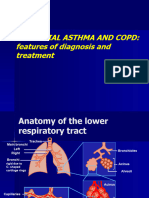
- 5 лекция БА и ХОБЛpptxDocument61 pages5 лекция БА и ХОБЛpptxdrsunil278Pas encore d'évaluation
- Pneumonia For Ug-1Document30 pagesPneumonia For Ug-1PranavPas encore d'évaluation
- Dyspnea - DR AllenDocument50 pagesDyspnea - DR AllenalmiraerickaiPas encore d'évaluation
- PBL 2nd Sem Scenario 1Document164 pagesPBL 2nd Sem Scenario 1stephaniecaronan15Pas encore d'évaluation
- Objectives: Table 1. Selected Etiologies of Sore ThroatDocument12 pagesObjectives: Table 1. Selected Etiologies of Sore ThroatRANIPas encore d'évaluation
- NCM 112 Respiratory HandoutDocument7 pagesNCM 112 Respiratory HandoutissaiahnicollePas encore d'évaluation
- Adult PathophysiologyDocument163 pagesAdult PathophysiologyRuthaliya IbrahimPas encore d'évaluation
- Lower Airway Obstruction and BronchiolitisDocument5 pagesLower Airway Obstruction and BronchiolitisGulrejPas encore d'évaluation
- This Young Man Has Long History of Productive Cough and Wheezing. He Is Afebrile and Chest Auscultation Reveals Coarse Crackles at Right Lower ChestDocument57 pagesThis Young Man Has Long History of Productive Cough and Wheezing. He Is Afebrile and Chest Auscultation Reveals Coarse Crackles at Right Lower ChestdrstraoPas encore d'évaluation
- Chronic Dry CoughDocument119 pagesChronic Dry CoughUzma KhanPas encore d'évaluation
- Seminar ChildDocument28 pagesSeminar ChildAung Khaing MoePas encore d'évaluation
- Internal Medicine Table SummaryDocument31 pagesInternal Medicine Table SummaryShazaan Nadeem100% (1)
- The System: RespiDocument219 pagesThe System: Respilalaine22dale100% (1)
- Bronchiolitis: Sarit Levinsky Maxim Melomud Group M1656Document23 pagesBronchiolitis: Sarit Levinsky Maxim Melomud Group M1656Sarit LevinskyPas encore d'évaluation
- PALS (Pediatric Advanced Life Support)Document48 pagesPALS (Pediatric Advanced Life Support)Jackson HakimPas encore d'évaluation
- Respiratory System NotesDocument85 pagesRespiratory System NotesMark Lorenz NaldozaPas encore d'évaluation
- Emergency Medicine Fourth Problem: Group 09 Tuesday, October 15, 2019Document47 pagesEmergency Medicine Fourth Problem: Group 09 Tuesday, October 15, 2019waraney palitPas encore d'évaluation
- LIMITLESS PEDIATRICS BY DR NAVEEN - DAY 4 (Green)Document56 pagesLIMITLESS PEDIATRICS BY DR NAVEEN - DAY 4 (Green)Biplav SinghPas encore d'évaluation
- BBDM Skenario 4 Modul 4.1 - DD (Bronkiektasis Dan Bronkitis Kronik)Document14 pagesBBDM Skenario 4 Modul 4.1 - DD (Bronkiektasis Dan Bronkitis Kronik)annisaPas encore d'évaluation
- Notes EntDocument43 pagesNotes Entadriana azmanPas encore d'évaluation
- Disturbances in OxygenationDocument10 pagesDisturbances in OxygenationjenrylPas encore d'évaluation
- MED - Interstitial Lung Disease, Final Sept08Document91 pagesMED - Interstitial Lung Disease, Final Sept08api-3856051100% (3)
- Objectives: Table 1. Selected Etiologies of Sore ThroatDocument12 pagesObjectives: Table 1. Selected Etiologies of Sore ThroatRiadi riadiPas encore d'évaluation
- ASTHMA CPD FINAL (Autosaved)Document74 pagesASTHMA CPD FINAL (Autosaved)Affri Dian AdiyatnaPas encore d'évaluation
- Calvin K.W. Tong Approach To A Child With A Cough: General PresentationDocument5 pagesCalvin K.W. Tong Approach To A Child With A Cough: General Presentationromeoenny4154Pas encore d'évaluation
- TB SutDocument17 pagesTB SutVivek TiwariPas encore d'évaluation
- Microbial Diseases of The Respiratory SystemDocument37 pagesMicrobial Diseases of The Respiratory SystemKristine Angie RamosPas encore d'évaluation
- Clinically Proven NutritionDocument16 pagesClinically Proven Nutritiongalihmd07Pas encore d'évaluation
- Child's NosebleedsDocument29 pagesChild's Nosebleedsgalihmd07Pas encore d'évaluation
- SEPSIS Guideline + EGDT of PedDocument33 pagesSEPSIS Guideline + EGDT of PedBorwon WittayaPas encore d'évaluation
- Fluidos Pasar A 5 A 10 Min Vs Pasar A 20 MinDocument11 pagesFluidos Pasar A 5 A 10 Min Vs Pasar A 20 MinRudy SanabriaPas encore d'évaluation
- Pediatric Acute Transverse MyelitisDocument8 pagesPediatric Acute Transverse Myelitisgalihmd07Pas encore d'évaluation
- High N Low Dose Ivig On GbsDocument9 pagesHigh N Low Dose Ivig On Gbsgalihmd07Pas encore d'évaluation
- Resume Abdullah AljufayrDocument5 pagesResume Abdullah AljufayrAbdullah SalehPas encore d'évaluation
- Fisher Divorce Adjustment Scale - Scoring GuideDocument7 pagesFisher Divorce Adjustment Scale - Scoring GuidecioconabegailPas encore d'évaluation
- Qlik Sense Architecture - Magnus BergDocument48 pagesQlik Sense Architecture - Magnus BergBạch HạcPas encore d'évaluation
- Writers Craft LP - Day 1Document9 pagesWriters Craft LP - Day 1api-357297274Pas encore d'évaluation
- Ucsp Tos First QuarterlyDocument8 pagesUcsp Tos First QuarterlyJuvelyn AbuganPas encore d'évaluation
- Youth Day EssayDocument1 pageYouth Day Essay6Master CryptoPas encore d'évaluation
- Java-Project Title 2021Document6 pagesJava-Project Title 2021HelloprojectPas encore d'évaluation
- 2013 12 Dec PaybillDocument121 pages2013 12 Dec Paybillapi-276412679Pas encore d'évaluation
- Danielle Nava: Harvard Human Rights JournalDocument1 pageDanielle Nava: Harvard Human Rights JournalfdxgfdgbfbhPas encore d'évaluation
- Subiect Engleza Clasa5Document3 pagesSubiect Engleza Clasa5Nelu Stoica100% (3)
- Orientation For The Opening of Class FOR KINDER-GRADE 3 S.Y 2020-2021Document8 pagesOrientation For The Opening of Class FOR KINDER-GRADE 3 S.Y 2020-2021LALA MAHALPas encore d'évaluation
- TFN Finals ExamDocument9 pagesTFN Finals ExamAlthea Aubrey AgbayaniPas encore d'évaluation
- Adm201 Chapter 1 PersonalityDocument46 pagesAdm201 Chapter 1 PersonalityIsmail AizatPas encore d'évaluation
- Assignment 6: Descriptive StatisticsDocument4 pagesAssignment 6: Descriptive StatisticsKrisna Dharma PutraPas encore d'évaluation
- I. Choose The Best AnswerDocument6 pagesI. Choose The Best AnswerGa MusaPas encore d'évaluation
- Experiments With An Axial Fan: Page 1/3 10/2010Document3 pagesExperiments With An Axial Fan: Page 1/3 10/2010Priyam ParasharPas encore d'évaluation
- Facebook Addiction and Academic Anxiety Among University StudentsDocument16 pagesFacebook Addiction and Academic Anxiety Among University StudentsLawson SohPas encore d'évaluation
- Adoc - Pub - The Japanese Language Proficiency Test Minggu 4 deDocument24 pagesAdoc - Pub - The Japanese Language Proficiency Test Minggu 4 deSushi Ikan32Pas encore d'évaluation
- Discursive Strategies of - Purity of Blood - in The First New Chronicle and Good Government by Felipe Guaman Poma de AyalaDocument97 pagesDiscursive Strategies of - Purity of Blood - in The First New Chronicle and Good Government by Felipe Guaman Poma de AyalaFlorin TanasoiuPas encore d'évaluation
- Programme Book HIPDocument2 pagesProgramme Book HIPAmira RodzizanPas encore d'évaluation
- Mba Finance CourseworkDocument7 pagesMba Finance Courseworkbcrqs9hr100% (2)
- Tally ERP9 by Dr.P.rizwan AhmedDocument8 pagesTally ERP9 by Dr.P.rizwan AhmedRizwan Ahmed100% (1)
- Domicile Under International LawDocument11 pagesDomicile Under International LawLEX 4790% (10)
- Local Literature Thesis WritingDocument7 pagesLocal Literature Thesis Writingzyxnlmikd100% (1)
- Lessons and Activities On Apartheid DBQDocument25 pagesLessons and Activities On Apartheid DBQChaii Madlangsakay Tolentino100% (1)
- Predictive Maintenance Ebook All ChaptersDocument58 pagesPredictive Maintenance Ebook All ChaptersMohamed taha EL M'HAMDIPas encore d'évaluation
- Predicting Student Academic Performance in Blended Learning Using Artificial Neural Networks Full TextDocument13 pagesPredicting Student Academic Performance in Blended Learning Using Artificial Neural Networks Full TextAdam HansenPas encore d'évaluation
- The Moi Formula For Improper Algebraic-Exponential IntegralDocument5 pagesThe Moi Formula For Improper Algebraic-Exponential IntegralFrank Waabu O'Brien (Dr. Francis J. O'Brien Jr.)Pas encore d'évaluation