Vous aimerez peut-être aussi
- Lean and CleanDocument146 pagesLean and CleanDavid Robson94% (18)
- Antenatal RecordDocument7 pagesAntenatal RecordDoxo Rubicin100% (2)
- RuckingDocument22 pagesRuckingLinming Ho100% (1)
- Sample ResumeDocument3 pagesSample Resumeapi-380209683% (6)
- UAS Genap B.ing-XI.2018Document15 pagesUAS Genap B.ing-XI.2018Slamet Munawar33% (3)
- Bland DietDocument17 pagesBland DietAdade Solomon Yao-Say100% (1)
- Electrolytes and Minerals/Acid Base Common Serum Enzymes: Table 8-1Document1 pageElectrolytes and Minerals/Acid Base Common Serum Enzymes: Table 8-1JUSASBPas encore d'évaluation
- Generic Name Brand Names Common Uses Possible Side Effects Mechanism of ActionDocument13 pagesGeneric Name Brand Names Common Uses Possible Side Effects Mechanism of Actionangel3424Pas encore d'évaluation
- Antidotes: Poison/Drug AntidoteDocument1 pageAntidotes: Poison/Drug AntidoteAfsal Ur FriendPas encore d'évaluation
- Cal Pharmaspirit PH Cal Q ADocument49 pagesCal Pharmaspirit PH Cal Q AAriadne BalmacedaPas encore d'évaluation
- Test 10Document2 pagesTest 10Shan ShaniPas encore d'évaluation
- M. Pharm Review NAPLEX38Document1 pageM. Pharm Review NAPLEX38JUSASBPas encore d'évaluation
- Cardiovascular Diagnostic Tests & Procedures.Document25 pagesCardiovascular Diagnostic Tests & Procedures.Salman KhanPas encore d'évaluation
- M. Pharm Review NAPLEX36Document1 pageM. Pharm Review NAPLEX36JUSASBPas encore d'évaluation
- M. Pharm Review NAPLEX07Document1 pageM. Pharm Review NAPLEX07JUSASBPas encore d'évaluation
- HAAD Applicant KitDocument9 pagesHAAD Applicant KitMenGuitarPas encore d'évaluation
- Pre Assessment Diabetes Nursing CareDocument4 pagesPre Assessment Diabetes Nursing CareHabib UllahPas encore d'évaluation
- Challenges in Hypertension ManagementDocument86 pagesChallenges in Hypertension ManagementAdel SALLAMPas encore d'évaluation
- AMH Must FlagDocument2 pagesAMH Must FlagpurnibaPas encore d'évaluation
- M. Pharm Review NAPLEX32Document1 pageM. Pharm Review NAPLEX32JUSASBPas encore d'évaluation
- Pharmacovigilance DefinationsDocument32 pagesPharmacovigilance DefinationsKadir AmirPas encore d'évaluation
- Classification of The DrugsDocument50 pagesClassification of The DrugsGlena SalamPas encore d'évaluation
- Vitamins & Minerals: Slam Shraf AhmyDocument5 pagesVitamins & Minerals: Slam Shraf AhmyAfsal Ur FriendPas encore d'évaluation
- SPLE Q ADocument90 pagesSPLE Q AZahra Ahmed AlzaherPas encore d'évaluation
- Resistant Hypertension. AHADocument38 pagesResistant Hypertension. AHAEderEmmanuelMartinezRuiz100% (1)
- COPD ExacerbationDocument2 pagesCOPD ExacerbationjusthoangPas encore d'évaluation
- 2017 April Exam CompilationDocument8 pages2017 April Exam CompilationabbasyaqobiPas encore d'évaluation
- WHO MDR 2020 Handbook Treatment PDFDocument88 pagesWHO MDR 2020 Handbook Treatment PDFYuanita GunawanPas encore d'évaluation
- M. Pharm Review NAPLEX28Document1 pageM. Pharm Review NAPLEX28JUSASBPas encore d'évaluation
- Top 10 Drug InteractionsDocument4 pagesTop 10 Drug InteractionsLeyla MajundaPas encore d'évaluation
- Antidotes and The Clinical Applications Antidote: An Antidote Is A Substance Which Can Counteract A Form ofDocument2 pagesAntidotes and The Clinical Applications Antidote: An Antidote Is A Substance Which Can Counteract A Form ofManohar Chowdary KovvuriPas encore d'évaluation
- lec2 المعدلةDocument120 pageslec2 المعدلةAhmed FouadPas encore d'évaluation
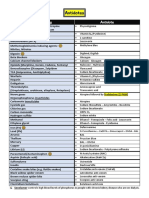
- Antibiotics Classification Guide for Penicillins, Cephalosporins, Fluoroquinolones and MoreDocument1 pageAntibiotics Classification Guide for Penicillins, Cephalosporins, Fluoroquinolones and MorestarobinPas encore d'évaluation
- Practice Test # 01 (Past Year PPSC Paper) : JOIN IS at WHATSAPP +92 333 2243031Document19 pagesPractice Test # 01 (Past Year PPSC Paper) : JOIN IS at WHATSAPP +92 333 2243031Saima ShehzadPas encore d'évaluation
- NORADRENALINE (Norepinephrine) : Presentation DescriptionDocument3 pagesNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraPas encore d'évaluation
- Pharmaco GenomicsDocument4 pagesPharmaco GenomicsFahad AlkenaniPas encore d'évaluation
- 15 - April - 2018: C-Fendaparinux + Low Molecular Weight HeparinDocument8 pages15 - April - 2018: C-Fendaparinux + Low Molecular Weight HeparinAbdul SalamPas encore d'évaluation
- Pharm MnemonicsDocument47 pagesPharm MnemonicsMina RacadioPas encore d'évaluation
- Hypertension Treatment Steps For HypertensionDocument15 pagesHypertension Treatment Steps For Hypertensionfreelancer08100% (1)
- Medication ErrorsDocument2 pagesMedication ErrorsFahad AlkenaniPas encore d'évaluation
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiPas encore d'évaluation
- (9-10-11 2022)Document173 pages(9-10-11 2022)SEIYADU IBRAHIM KPas encore d'évaluation
- Oman Prometric Exam Notes: Download NowDocument16 pagesOman Prometric Exam Notes: Download NowneethuPas encore d'évaluation
- GUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامDocument1 pageGUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامAbu HuzaifaPas encore d'évaluation
- PharmaDocument10 pagesPharmaSEIYADU IBRAHIM KPas encore d'évaluation
- 3 - March 2021Document116 pages3 - March 2021SEIYADU IBRAHIM KPas encore d'évaluation
- Drug Interactions of Antianginal Drugs..Document40 pagesDrug Interactions of Antianginal Drugs..Kamal SikandarPas encore d'évaluation
- 2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDDocument58 pages2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDKishan SethPas encore d'évaluation
- QuestionsDocument13 pagesQuestionsMikee MeladPas encore d'évaluation
- Prescription Writing HypertensionDocument18 pagesPrescription Writing HypertensionSAHILA SHEIKHPas encore d'évaluation
- Pharmacology of Drugs For AnemiaDocument49 pagesPharmacology of Drugs For AnemiaTeus Fatamorgana100% (2)
- Ed enDocument376 pagesEd enNashria Rusdhy100% (2)
- Pharmacology Questions1Document2 pagesPharmacology Questions1أبوأحمد الحكيمPas encore d'évaluation
- Side EffectsDocument2 pagesSide EffectsFahad AlkenaniPas encore d'évaluation
- APHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDocument13 pagesAPHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDrSamia El WakilPas encore d'évaluation
- Cap 4-5-6 Painkillers, Local and Gen Anest - 2020Document15 pagesCap 4-5-6 Painkillers, Local and Gen Anest - 2020Irina Panciu StefanPas encore d'évaluation
- A) AcetylationDocument4 pagesA) Acetylationvara prasadPas encore d'évaluation
- 417 QDocument41 pages417 QfaisalnadeemPas encore d'évaluation
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تPas encore d'évaluation
- New Question for MoH Prometric Exam تمDocument7 pagesNew Question for MoH Prometric Exam تمsundus951100% (1)
- Sem 5/unit-3 Autocoids & Related DrugsDocument28 pagesSem 5/unit-3 Autocoids & Related DrugsDARSHAN BhirudPas encore d'évaluation
- ASNAN FINAL MCQs PART I PDFDocument21 pagesASNAN FINAL MCQs PART I PDFNasser Hashim0% (1)
- Beta Blockers: ExampleDocument9 pagesBeta Blockers: ExampletiaraPas encore d'évaluation
- CardiovascularDocument28 pagesCardiovascularFarhan AbdiPas encore d'évaluation
- Migraine: By: B K PandaDocument19 pagesMigraine: By: B K PandapandabijoyPas encore d'évaluation
- Study of Clinical Efficacy, Safety and Tolerability of Low Cost Branded Generic Antiepileptic Drugs in Children and AdolescentsDocument6 pagesStudy of Clinical Efficacy, Safety and Tolerability of Low Cost Branded Generic Antiepileptic Drugs in Children and AdolescentspandabijoyPas encore d'évaluation
- Study of Clinical Efficacy, Safety and Tolerability of Low Cost Branded Generic Antiepileptic Drugs in Children and AdolescentsDocument6 pagesStudy of Clinical Efficacy, Safety and Tolerability of Low Cost Branded Generic Antiepileptic Drugs in Children and AdolescentspandabijoyPas encore d'évaluation
- Study of Clinical Efficacy, Safety and Tolerability of Low Cost Branded Generic Antiepileptic Drugs in Children and AdolescentsDocument6 pagesStudy of Clinical Efficacy, Safety and Tolerability of Low Cost Branded Generic Antiepileptic Drugs in Children and AdolescentspandabijoyPas encore d'évaluation
- Clinical Trials PhasesDocument2 pagesClinical Trials PhasespandabijoyPas encore d'évaluation
- Clinical Pharmacists in Emergency MedicineDocument12 pagesClinical Pharmacists in Emergency MedicinepandabijoyPas encore d'évaluation
- LI References StyleDocument23 pagesLI References StyleimnaliniPas encore d'évaluation
- Linking Ideas and Academic WritingDocument7 pagesLinking Ideas and Academic Writingoliver cotaquispePas encore d'évaluation
- How To Use Ketovatru Supplement?Document5 pagesHow To Use Ketovatru Supplement?velofel usesPas encore d'évaluation
- Medical Tribune July 2012 HKDocument88 pagesMedical Tribune July 2012 HKKarena SabadoPas encore d'évaluation
- Pcol MnemonicsDocument12 pagesPcol MnemonicsJustine Rubillete Mendoza MarianoPas encore d'évaluation
- According To The Study of Len KravitzDocument4 pagesAccording To The Study of Len KravitzRon NecesitoPas encore d'évaluation
- Sugar Myths 1 KMUD 2011Document14 pagesSugar Myths 1 KMUD 2011Eric JohnsonPas encore d'évaluation
- HTN BrochureDocument2 pagesHTN Brochureapi-400548889Pas encore d'évaluation
- Trans Fats Health and Nutritional Labeling of FoodsDocument2 pagesTrans Fats Health and Nutritional Labeling of FoodsJohn Henry WellsPas encore d'évaluation
- Choose My Plate ProjectDocument3 pagesChoose My Plate Projectapi-309612338Pas encore d'évaluation
- Pathfit 1 Module 12 Week 14Document2 pagesPathfit 1 Module 12 Week 14Mark Anthony RabyPas encore d'évaluation
- Essie Hoiball and T.C. Fry - I Live On Fruit (1981)Document40 pagesEssie Hoiball and T.C. Fry - I Live On Fruit (1981)Charles100% (11)
- Uppercut MagazineDocument12 pagesUppercut MagazineChris Finn100% (1)
- Lesson 2 q1 P.E. Active RecreationDocument79 pagesLesson 2 q1 P.E. Active RecreationIleneah BenchPas encore d'évaluation
- Benefits of TriphalaDocument4 pagesBenefits of TriphalaAditya Sharma100% (1)
- Carbohydrate: N) - However, Not All Carbohydrates Conform To ThisDocument13 pagesCarbohydrate: N) - However, Not All Carbohydrates Conform To ThisCrow LordPas encore d'évaluation
- Cabbage Soup Recipe: Day OneDocument5 pagesCabbage Soup Recipe: Day OneJacob JayaseelanPas encore d'évaluation
- Nonalcoholic Fatty Liver Disease (Nafld)Document35 pagesNonalcoholic Fatty Liver Disease (Nafld)FUTURE DOCTOR100% (1)
- Burs Lem 2021Document13 pagesBurs Lem 2021ERINSONPas encore d'évaluation
- 9 - Oils and FatsDocument9 pages9 - Oils and FatsUvvj RajuPas encore d'évaluation
- HDHK 1Document26 pagesHDHK 1swaftyPas encore d'évaluation
- Power 0304 2012 PDFDocument60 pagesPower 0304 2012 PDFAnonymous O7NI8R3gFAPas encore d'évaluation
- STEP HPEF Trial NEJm 2023Document16 pagesSTEP HPEF Trial NEJm 2023felipePas encore d'évaluation
- SetyaningrumrahmawatyDocument3 pagesSetyaningrumrahmawatyBoh Cucu KaraengPas encore d'évaluation
- Hungarian meals and dining customsDocument3 pagesHungarian meals and dining customsonodiivettPas encore d'évaluation
- PS EseDocument3 pagesPS EseAsh KPas encore d'évaluation