Vous aimerez peut-être aussi
- Urinalysis 150313040235 Conversion Gate01Document30 pagesUrinalysis 150313040235 Conversion Gate01AbhishiktaAbhi100% (1)
- UrinalysisDocument61 pagesUrinalysisMohammed AyaleqPas encore d'évaluation
- Renal Function Test Amcj 8Document42 pagesRenal Function Test Amcj 8Md. Saifur Rahman SunnyPas encore d'évaluation
- Physical Characteristics of UrineDocument36 pagesPhysical Characteristics of Urinemuhammad saad100% (1)
- Lab 9++10 Pathological UrinlysisDocument38 pagesLab 9++10 Pathological UrinlysisSai SreedharPas encore d'évaluation
- Urinalysis in The Diagnosis of Kidney DiseaseDocument94 pagesUrinalysis in The Diagnosis of Kidney DiseasegibreilPas encore d'évaluation
- Microscopic Urinalysis GuideDocument37 pagesMicroscopic Urinalysis GuideM. JoycePas encore d'évaluation
- 4 - Urine BenchDocument37 pages4 - Urine BenchChiizu iraPas encore d'évaluation
- Urine Analysis PracticalDocument53 pagesUrine Analysis PracticalMubasharAbrar100% (2)
- UrinalysisDocument32 pagesUrinalysiskholoud220Pas encore d'évaluation
- Urinalysis Tests ExplainedDocument14 pagesUrinalysis Tests ExplainedAl- ImanuddinPas encore d'évaluation
- Art and Science of UrinalysisDocument31 pagesArt and Science of UrinalysisTia AriantiPas encore d'évaluation
- Chemical Examination of UrineDocument32 pagesChemical Examination of UrineMarti DeanePas encore d'évaluation
- General Urine Analysis GuideDocument24 pagesGeneral Urine Analysis GuideQasmPas encore d'évaluation
- Diagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical ExaminationDocument58 pagesDiagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical Examinationsanjay kumarPas encore d'évaluation
- Urine Full Exam and Microscopic Exam (UrinalysisDocument11 pagesUrine Full Exam and Microscopic Exam (UrinalysisKarthigaRamanPas encore d'évaluation
- Clinical Analytical MethodsDocument47 pagesClinical Analytical MethodsDesta Yakob Doda 18BML0121Pas encore d'évaluation
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiPas encore d'évaluation
- Urine Analysis: Assist. Prof. Biochemistry Dep., Faculty of Medicine Asu & UqDocument21 pagesUrine Analysis: Assist. Prof. Biochemistry Dep., Faculty of Medicine Asu & UqArjunaPamungkasPas encore d'évaluation
- Macroscopic UrinalysisDocument29 pagesMacroscopic UrinalysisJames De VeraPas encore d'évaluation
- Urinalysis - Fundamentals of Nursing CliDocument30 pagesUrinalysis - Fundamentals of Nursing CliJessica BeanPas encore d'évaluation
- Urine AnalysisDocument41 pagesUrine AnalysisAjay SomeshwarPas encore d'évaluation
- Biochemistry of Urine: By: Jerome S. Montano, RMTDocument28 pagesBiochemistry of Urine: By: Jerome S. Montano, RMTAhuPas encore d'évaluation
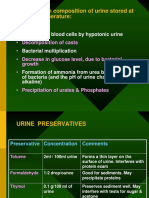
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarPas encore d'évaluation
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaPas encore d'évaluation
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomPas encore d'évaluation
- Urine Analysis Results and Microscopic FindingsDocument30 pagesUrine Analysis Results and Microscopic FindingsMeera NandanPas encore d'évaluation
- Kidney Function and Urine AnalysisDocument42 pagesKidney Function and Urine AnalysisajaysomPas encore d'évaluation
- Clinical Biochemistry Tests for Disease Diagnosis and MonitoringDocument25 pagesClinical Biochemistry Tests for Disease Diagnosis and MonitoringTennidoxPas encore d'évaluation
- Urine Analysis FinalDocument112 pagesUrine Analysis FinalNischita JayarajPas encore d'évaluation
- Lesson 15 Fecalysis and Gastric AnalysisDocument39 pagesLesson 15 Fecalysis and Gastric AnalysisFaith TambongPas encore d'évaluation
- Urinalysis PDFDocument56 pagesUrinalysis PDFTio AjhaPas encore d'évaluation
- Obstructive Jaundice: DR Nanteza SumayiyaDocument26 pagesObstructive Jaundice: DR Nanteza SumayiyaNinaPas encore d'évaluation
- Pharmacy Skills Lecture 7Document25 pagesPharmacy Skills Lecture 7Rabab Hamed SayedPas encore d'évaluation
- Blood AnalysisDocument10 pagesBlood AnalysisHry WkPas encore d'évaluation
- Clinical analytical methods: Hemocytometer, urine analysis, liver and kidney function testsDocument47 pagesClinical analytical methods: Hemocytometer, urine analysis, liver and kidney function testsCathrine CruzPas encore d'évaluation
- Pharmd - 4Y & 1Y (PB) - 4.3 - Clinical PharmacyDocument24 pagesPharmd - 4Y & 1Y (PB) - 4.3 - Clinical PharmacyDebasish SanyalPas encore d'évaluation
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocument49 pagesUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshPas encore d'évaluation
- Clinical Case On JaundiceDocument43 pagesClinical Case On JaundicePro fatherPas encore d'évaluation
- Somaville University Faculty of Medicine Urology &Nephrology Lecturer: Dr.Osman Urine Analyze Presentation By Group ADocument49 pagesSomaville University Faculty of Medicine Urology &Nephrology Lecturer: Dr.Osman Urine Analyze Presentation By Group ALayla CabduqaadirPas encore d'évaluation
- Urinalysis and Body Fluids2020Document47 pagesUrinalysis and Body Fluids2020MONFOLA100% (1)
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 pagesRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomPas encore d'évaluation
- Approach To ProteinuriaDocument35 pagesApproach To ProteinuriaKebede TesfayePas encore d'évaluation
- Complete Urinalysis: A. Physical Characteristics of UrineDocument8 pagesComplete Urinalysis: A. Physical Characteristics of UrineKryza Dale Bunado BaticanPas encore d'évaluation
- UrinsryDocument10 pagesUrinsryAzizan HakimPas encore d'évaluation
- Biochemistry of Jaundice Group 2 FinalDocument44 pagesBiochemistry of Jaundice Group 2 FinalShanna SolideoPas encore d'évaluation
- URINALYSIS TESTING GUIDEDocument6 pagesURINALYSIS TESTING GUIDEThanz Pamela Gargueña Guisihan100% (1)
- JaundiceDocument29 pagesJaundiceMurali TiarasanPas encore d'évaluation
- Clinical Pathology Fecalysis and UrnalysisDocument16 pagesClinical Pathology Fecalysis and UrnalysisRem Alfelor100% (3)
- Jaundie 2Document25 pagesJaundie 2Nambuye Midyero AhmedPas encore d'évaluation
- Rine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al MaqadmaDocument39 pagesRine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al Maqadmaiman zainuddinPas encore d'évaluation
- Analysis of Urine Constituents & Abnormal Findings (39Document74 pagesAnalysis of Urine Constituents & Abnormal Findings (39sabao kizuitePas encore d'évaluation
- UrineDocument52 pagesUrineMohammed Tahoun100% (1)
- 50, 51. Diseases of The Equine Urinary TractDocument20 pages50, 51. Diseases of The Equine Urinary TractNatalie HowardPas encore d'évaluation
- Urinary Symptoms - DR RashaDocument70 pagesUrinary Symptoms - DR RashaRasha TelebPas encore d'évaluation
- Expected urine test results and significance of key diagnostic markersDocument2 pagesExpected urine test results and significance of key diagnostic markersmrvictor008Pas encore d'évaluation
- URINALYSISDocument80 pagesURINALYSISredr7131Pas encore d'évaluation
- Common Laboratory Tests:: Body FluidsDocument37 pagesCommon Laboratory Tests:: Body FluidsmujPas encore d'évaluation
- Urine AnalysisDocument53 pagesUrine AnalysisMaath KhalidPas encore d'évaluation
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisD'EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisÉvaluation : 3 sur 5 étoiles3/5 (1)
- Growth Disorders, Differentiation, and MorphogenesisDocument4 pagesGrowth Disorders, Differentiation, and MorphogenesisDapot SianiparPas encore d'évaluation
- Bone Metabolism: German VersionDocument17 pagesBone Metabolism: German VersionDapot SianiparPas encore d'évaluation
- Lecture TemperatureDocument47 pagesLecture TemperatureDapot SianiparPas encore d'évaluation
- Lab Physiology 1Document2 pagesLab Physiology 1Dapot SianiparPas encore d'évaluation
- MCQ FMS 2 BATCH 2016 Bone and Calcium HomeostasisDocument20 pagesMCQ FMS 2 BATCH 2016 Bone and Calcium Homeostasisstella pangestikaPas encore d'évaluation
- Tugas Upper 0 Lowe Limb MusclesDocument17 pagesTugas Upper 0 Lowe Limb MusclesDapot SianiparPas encore d'évaluation
- Exp. Week 4Document2 pagesExp. Week 4Dapot SianiparPas encore d'évaluation
- FMS III WO Week 5Document6 pagesFMS III WO Week 5Dapot SianiparPas encore d'évaluation
- Exp. Week 4Document2 pagesExp. Week 4Dapot SianiparPas encore d'évaluation
- Introduction To History Taking: Lecturer: Dr. Theo Audiyanto, Sp. PDDocument26 pagesIntroduction To History Taking: Lecturer: Dr. Theo Audiyanto, Sp. PDDapot SianiparPas encore d'évaluation
- TO 2 Anatomy 2016Document10 pagesTO 2 Anatomy 2016Dapot SianiparPas encore d'évaluation
- Why Doctors Get SuedDocument7 pagesWhy Doctors Get SuedDapot SianiparPas encore d'évaluation
- Humoral Component of The Immune SystemDocument13 pagesHumoral Component of The Immune SystemDapot SianiparPas encore d'évaluation
- MCQ FMS 2Document19 pagesMCQ FMS 2Dapot SianiparPas encore d'évaluation
- MCQ FMS 2 BATCH 2016 Bone and Calcium HomeostasisDocument20 pagesMCQ FMS 2 BATCH 2016 Bone and Calcium Homeostasisstella pangestikaPas encore d'évaluation
- FMS II Lab Manual Week 1Document20 pagesFMS II Lab Manual Week 1Dapot SianiparPas encore d'évaluation
- Oncologic Emergencies Hypercalcemia of MalignancyDocument6 pagesOncologic Emergencies Hypercalcemia of MalignancyDapot SianiparPas encore d'évaluation
- CS 1 - 2017 PDFDocument77 pagesCS 1 - 2017 PDFDapot SianiparPas encore d'évaluation
- LO Hemato 4.1Document9 pagesLO Hemato 4.1Dapot SianiparPas encore d'évaluation
- Oncologic Emergencies Hypercalcemia of MalignancyDocument6 pagesOncologic Emergencies Hypercalcemia of MalignancyDapot SianiparPas encore d'évaluation
- LO Hemato 5.2Document5 pagesLO Hemato 5.2Dapot SianiparPas encore d'évaluation
- Soal Compile Hemato-OncologyDocument25 pagesSoal Compile Hemato-OncologyDapot SianiparPas encore d'évaluation
- LO Hemato 5.1Document4 pagesLO Hemato 5.1Dapot SianiparPas encore d'évaluation
- HEMOPHILIA GuidelinesDocument76 pagesHEMOPHILIA Guidelinesmarco_jacinto1103197Pas encore d'évaluation
- HemophiliaDocument48 pagesHemophiliaDapot SianiparPas encore d'évaluation
- LO Hemato 3.1Document6 pagesLO Hemato 3.1Dapot SianiparPas encore d'évaluation
- LO TambahanDocument5 pagesLO TambahanDapot SianiparPas encore d'évaluation
- Lecture BB 2018Document2 pagesLecture BB 2018Dapot SianiparPas encore d'évaluation
- LO Hemato 2Document8 pagesLO Hemato 2Dapot SianiparPas encore d'évaluation
- Baca RabuDocument1 pageBaca RabuDapot SianiparPas encore d'évaluation
- NEC Article 250Document42 pagesNEC Article 250unknown_3100% (1)
- 171 - New CAN-filter For Cran Com. SCS4 and MidrangeDocument4 pages171 - New CAN-filter For Cran Com. SCS4 and MidrangeMohamed ElnagdyPas encore d'évaluation
- LC IN SCIENCE and MathDocument14 pagesLC IN SCIENCE and MathCharity Anne Camille PenalozaPas encore d'évaluation
- Service Manual: S&T Motors Co., LTDDocument94 pagesService Manual: S&T Motors Co., LTDJuliano PedrosoPas encore d'évaluation
- Is A Calorie Really A Calorie - Metabolic Advantage of Low-Carbohydrate DietsDocument6 pagesIs A Calorie Really A Calorie - Metabolic Advantage of Low-Carbohydrate DietsGustavo CastroPas encore d'évaluation
- Manual de Operacion de Bomba BlackmerDocument20 pagesManual de Operacion de Bomba BlackmerMorales EduardoPas encore d'évaluation
- Tradesman Electronics PDFDocument13 pagesTradesman Electronics PDFsandeepxrPas encore d'évaluation
- Notifier Battery Calculations-ReadmeDocument11 pagesNotifier Battery Calculations-ReadmeJeanCarlosRiveroPas encore d'évaluation
- Windows Mbox Viewer User Manual 1.0.3.4Document33 pagesWindows Mbox Viewer User Manual 1.0.3.4Billy NoelPas encore d'évaluation
- Kalayaan Elementary SchoolDocument3 pagesKalayaan Elementary SchoolEmmanuel MejiaPas encore d'évaluation
- Scoop Atlas Wagner ST1810Document4 pagesScoop Atlas Wagner ST1810Juan Manuel PerezPas encore d'évaluation
- 10th Term Exams Computer Science PaperDocument2 pages10th Term Exams Computer Science PaperMohammad Tariq JavaidPas encore d'évaluation
- ENGG1330 2N Computer Programming I (20-21 Semester 2) Assignment 1Document5 pagesENGG1330 2N Computer Programming I (20-21 Semester 2) Assignment 1Fizza JafferyPas encore d'évaluation
- Silo Cement CalculationDocument11 pagesSilo Cement CalculationFikriaraz AfifPas encore d'évaluation
- 13 - Wool-And-Coir-Fiber-Reinforced-Gypsum-Ceiling-Tiles-Wit - 2021 - Journal-of-BuilDocument9 pages13 - Wool-And-Coir-Fiber-Reinforced-Gypsum-Ceiling-Tiles-Wit - 2021 - Journal-of-BuilJenifer TejadaPas encore d'évaluation
- Xenomai 3 DocumentationDocument673 pagesXenomai 3 DocumentationGuile BonafiniPas encore d'évaluation
- Practice Workbook LR Method For Addition Subtraction PDFDocument4 pagesPractice Workbook LR Method For Addition Subtraction PDFEsa KhanPas encore d'évaluation
- HI-8592, HI-8593, HI-8594: Single-Rail ARINC 429 Differential Line DriverDocument14 pagesHI-8592, HI-8593, HI-8594: Single-Rail ARINC 429 Differential Line DriversameeppaiPas encore d'évaluation
- Curtis CatalogDocument9 pagesCurtis CatalogtharngalPas encore d'évaluation
- WR424GB00DDocument16 pagesWR424GB00DIgor San Martín PeñalozaPas encore d'évaluation
- Facilities Assignment 1-2-2015Document2 pagesFacilities Assignment 1-2-2015Xnort G. Xwest0% (1)
- Physical parameters shaping of Farwa Lagoon - LibyaDocument7 pagesPhysical parameters shaping of Farwa Lagoon - LibyaAsadeg ZaidPas encore d'évaluation
- Python Programming Lecture#2 - Functions, Lists, Packages & Formatting I/ODocument69 pagesPython Programming Lecture#2 - Functions, Lists, Packages & Formatting I/OHamsa VeniPas encore d'évaluation
- Astm A6 A6m-08Document62 pagesAstm A6 A6m-08Vũ Nhân HòaPas encore d'évaluation
- 1 05 Lab Crime Scene Sketch GADocument2 pages1 05 Lab Crime Scene Sketch GAthis is hardly gonna be usedPas encore d'évaluation
- SPPID QuestionsDocument2 pagesSPPID Questionsvivek83% (12)
- Ms-Dos Device Drivers: Device Drivers Are The That in File atDocument13 pagesMs-Dos Device Drivers: Device Drivers Are The That in File atJass GillPas encore d'évaluation
- VRV A 12 PDFDocument1 pageVRV A 12 PDFMoe Thiri ZunPas encore d'évaluation
- Qualcomm LTE Performance & Challenges 09-01-2011Document29 pagesQualcomm LTE Performance & Challenges 09-01-2011vembri2178100% (1)
- Product - 20V4000G24F 3B FODocument32 pagesProduct - 20V4000G24F 3B FOmohammed khadrPas encore d'évaluation