Vous aimerez peut-être aussi
- 13 16 Meeker IHC 9pDocument10 pages13 16 Meeker IHC 9pBrew-sam AB100% (1)
- MIRA 101, English, v14.1 PDFDocument4 pagesMIRA 101, English, v14.1 PDFNaee ARPas encore d'évaluation
- DIN EN 179 I 1125 PDFDocument3 pagesDIN EN 179 I 1125 PDFDushan RomicPas encore d'évaluation
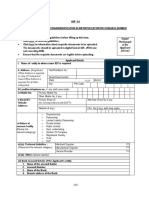
- Anf 2A: Office Address Is Required in Case of Companies/ Head Office Address Is Required For All Other Categories)Document4 pagesAnf 2A: Office Address Is Required in Case of Companies/ Head Office Address Is Required For All Other Categories)Dalu ChockiPas encore d'évaluation
- DT-1001 Ind RegDocument4 pagesDT-1001 Ind RegMugabi EltonbenPas encore d'évaluation
- The National Insurance Board of Trinidad and Tobago Maternity Benefit ApplicationDocument5 pagesThe National Insurance Board of Trinidad and Tobago Maternity Benefit ApplicationAriPas encore d'évaluation
- Company Limited Liability Re Registration FormDocument18 pagesCompany Limited Liability Re Registration FormNathaniel kobina QuainooPas encore d'évaluation
- FCB Acc OpeningAppFormCorporate 2Document12 pagesFCB Acc OpeningAppFormCorporate 2Matthew12Alexander12Pas encore d'évaluation
- Form GST REG-07: Government of India / State Government Department ofDocument4 pagesForm GST REG-07: Government of India / State Government Department ofthecoltPas encore d'évaluation
- Sample: Application Form Appointment of Distributors Information About YouDocument4 pagesSample: Application Form Appointment of Distributors Information About YouVenkateshPas encore d'évaluation
- (A) Director:: The Companies Act 1963 (Act 179)Document3 pages(A) Director:: The Companies Act 1963 (Act 179)Kwasi BoateyPas encore d'évaluation
- NGO Registration FormDocument14 pagesNGO Registration FormJoy Dake-AbrahamsPas encore d'évaluation
- ACE Palm FloorsDocument20 pagesACE Palm Floorsrahulsoni45Pas encore d'évaluation
- D-3949A Information Referral 072717Document3 pagesD-3949A Information Referral 072717niruhtPas encore d'évaluation
- Taxpayer Registration Form IndividualDocument4 pagesTaxpayer Registration Form IndividualAndy AsantePas encore d'évaluation
- MORONG Business Permit Form ARTADocument2 pagesMORONG Business Permit Form ARTAAz Khylle AlamonPas encore d'évaluation
- Application Form: Section A - Investor DetailsDocument3 pagesApplication Form: Section A - Investor Detailsmarianne10Pas encore d'évaluation
- 01 BPG - Customer Relationship Form - Non-IndividualDocument4 pages01 BPG - Customer Relationship Form - Non-IndividualchaudharyarvindPas encore d'évaluation
- Rev 2 - Change of Details EmailedDocument5 pagesRev 2 - Change of Details EmailedMunodawafa ChimhamhiwaPas encore d'évaluation
- Business Permit App FormDocument1 pageBusiness Permit App FormcheansiaPas encore d'évaluation
- Individuals: Account Opening Form For F. No.-401Document17 pagesIndividuals: Account Opening Form For F. No.-401Kishor AgrawalPas encore d'évaluation
- Application For Permanent Account Number (Pan) : IndividualsDocument3 pagesApplication For Permanent Account Number (Pan) : IndividualsBharat PangeniPas encore d'évaluation
- Pagsinag RA Forms March 2022Document15 pagesPagsinag RA Forms March 2022Angelica Perlyn AurelioPas encore d'évaluation
- Anf2a 2015Document4 pagesAnf2a 2015Vithani MehulPas encore d'évaluation
- Branch TINDocument3 pagesBranch TINJuma SaidPas encore d'évaluation
- EMP101 eDocument7 pagesEMP101 eNozipho MpofuPas encore d'évaluation
- City West WaterDocument1 pageCity West WaterRyanPas encore d'évaluation
- Form N 100 For Tanzanian LSSP Database February 2018Document11 pagesForm N 100 For Tanzanian LSSP Database February 2018SHANKARPas encore d'évaluation
- Arf - 2018Document6 pagesArf - 2018Vipin GargPas encore d'évaluation
- Tan 49 BDocument3 pagesTan 49 BTanu ThakurPas encore d'évaluation
- Employer Registration Form (Erf) : DD MM YYDocument2 pagesEmployer Registration Form (Erf) : DD MM YYManisha D ShiblollPas encore d'évaluation
- DTI TransportDocument5 pagesDTI Transport《Clarkyboy》 052017Pas encore d'évaluation
- Tarea 5Document9 pagesTarea 5josefaPas encore d'évaluation
- Taxpayer Registration Form OrganisationDocument4 pagesTaxpayer Registration Form OrganisationMagdalene AmewodzoPas encore d'évaluation
- SBP Prescribed Application Form For Governments Profit Subsidy Facility (English)Document6 pagesSBP Prescribed Application Form For Governments Profit Subsidy Facility (English)muhammadTzPas encore d'évaluation
- Application Form For Business PermitDocument13 pagesApplication Form For Business PermitKimBabPas encore d'évaluation
- City of Talisay: Requirements: 1. Brgy. Clearance 2. Dti/Sec/Cda 3. Sanitary Permit 4. OthersDocument1 pageCity of Talisay: Requirements: 1. Brgy. Clearance 2. Dti/Sec/Cda 3. Sanitary Permit 4. OthersDexter Q. JaducanaPas encore d'évaluation
- GST Registration FormDocument9 pagesGST Registration Formpankaj singlaPas encore d'évaluation
- Taxi and Private Hire Booking Office Licence Renewal Application ChecklistDocument8 pagesTaxi and Private Hire Booking Office Licence Renewal Application ChecklistAr. RajaPas encore d'évaluation
- Vendor Registration FormDocument15 pagesVendor Registration FormJTO-IT Manipur SSAPas encore d'évaluation
- Federal Board of Revenue Taxpayer Registration Form (V-2) : Current NTN (If Already Issued)Document5 pagesFederal Board of Revenue Taxpayer Registration Form (V-2) : Current NTN (If Already Issued)haseeb_javed_9Pas encore d'évaluation
- Undertaking Yedk146912967383Document5 pagesUndertaking Yedk146912967383karljaen87Pas encore d'évaluation
- Non Individual Taxpayer Registration FormDocument1 pageNon Individual Taxpayer Registration FormNwogboji EmmanuelPas encore d'évaluation
- Kotak NRE NRO Online AC Opening Customer Details - 2020-2021Document10 pagesKotak NRE NRO Online AC Opening Customer Details - 2020-2021KumarPas encore d'évaluation
- Information Referral: Department of The Treasury - Internal Revenue Service Form (12-2005) OMB # 1545-1960 (Document2 pagesInformation Referral: Department of The Treasury - Internal Revenue Service Form (12-2005) OMB # 1545-1960 (IRSPas encore d'évaluation
- F 13551Document2 pagesF 13551IRSPas encore d'évaluation
- Booking Office 3124Document8 pagesBooking Office 3124m227765hPas encore d'évaluation
- Republic of The Philippines Department of Trade and Industry Business Name Registration Sole Proprietorship Application FormDocument4 pagesRepublic of The Philippines Department of Trade and Industry Business Name Registration Sole Proprietorship Application FormJaime GonzalesPas encore d'évaluation
- Republic of The Philippines Department of Trade and Industry Business Name Registration Sole Proprietorship Application FormDocument4 pagesRepublic of The Philippines Department of Trade and Industry Business Name Registration Sole Proprietorship Application FormTIA BARTE FERRERPas encore d'évaluation
- Common Application Form: For Holding Units in Demat ModeDocument6 pagesCommon Application Form: For Holding Units in Demat ModevasucristalPas encore d'évaluation
- Undertaking Vsjo425514928209Document4 pagesUndertaking Vsjo425514928209jenelyn caminadePas encore d'évaluation
- Pan Card FormDocument3 pagesPan Card FormMehul ShahPas encore d'évaluation
- Information Referral: Form (2-2007) Department of The Treasury - Internal Revenue Service OMB # 1545-1960Document2 pagesInformation Referral: Form (2-2007) Department of The Treasury - Internal Revenue Service OMB # 1545-1960diversified1Pas encore d'évaluation
- Current Account Opening Form Single PDFDocument4 pagesCurrent Account Opening Form Single PDFSourabh TiwariPas encore d'évaluation
- PS 1583 Form SampleDocument1 pagePS 1583 Form SampleFenellaPas encore d'évaluation
- CLR - 004 - E - Application Form For Tax Clearance On Other PurposeDocument1 pageCLR - 004 - E - Application Form For Tax Clearance On Other PurposeRahul kumar SahPas encore d'évaluation
- Form No 49BDocument5 pagesForm No 49BVedant DistributorsPas encore d'évaluation
- How to Do a 1031 Exchange of Real Estate: Using a 1031 Qualified Intermediary (Qi) 2Nd EditionD'EverandHow to Do a 1031 Exchange of Real Estate: Using a 1031 Qualified Intermediary (Qi) 2Nd EditionPas encore d'évaluation
- Drafting Legal Notices in India: A Guide to Understanding the Importance of Legal Notices, along with DraftsD'EverandDrafting Legal Notices in India: A Guide to Understanding the Importance of Legal Notices, along with DraftsÉvaluation : 1 sur 5 étoiles1/5 (2)
- The Face Looking Company: The Beginning Love Walk Around the WorldD'EverandThe Face Looking Company: The Beginning Love Walk Around the WorldPas encore d'évaluation
- A Guide to District Court Civil Forms in the State of HawaiiD'EverandA Guide to District Court Civil Forms in the State of HawaiiPas encore d'évaluation
- Trennliste EnglischDocument2 pagesTrennliste EnglischBrew-sam ABPas encore d'évaluation
- High-Dose Thiamine and Essential Tremor: Antonio CostantiniDocument4 pagesHigh-Dose Thiamine and Essential Tremor: Antonio CostantiniBrew-sam ABPas encore d'évaluation
- And Molecular Mechanisms: Biological Clocks: Behavioural CharacteristicsDocument53 pagesAnd Molecular Mechanisms: Biological Clocks: Behavioural CharacteristicsBrew-sam ABPas encore d'évaluation
- Project 610530 Epp 1 2019 1 FR Eppka1 JMD MobDocument2 pagesProject 610530 Epp 1 2019 1 FR Eppka1 JMD MobBrew-sam ABPas encore d'évaluation
- Bookshelf NBK11546Document24 pagesBookshelf NBK11546Brew-sam ABPas encore d'évaluation
- FS Meeting20170425Document1 pageFS Meeting20170425Brew-sam ABPas encore d'évaluation
- 5 Point and Click Preprocessing2017Document13 pages5 Point and Click Preprocessing2017Brew-sam ABPas encore d'évaluation
- Book 5Document3 pagesBook 5Brew-sam ABPas encore d'évaluation
- Exam Biology StudentsDocument2 pagesExam Biology StudentsBrew-sam ABPas encore d'évaluation
- Living Language Ultimate German I PDFDocument437 pagesLiving Language Ultimate German I PDFBrew-sam AB100% (4)
- Winter Term 2017 / 2018: Planned Time Slots MSC Neuroscience Modules Plese Check Website and Stud - Ip For Updates!Document1 pageWinter Term 2017 / 2018: Planned Time Slots MSC Neuroscience Modules Plese Check Website and Stud - Ip For Updates!Brew-sam ABPas encore d'évaluation
- Cornelsen Einstufung Test (Abraham Brew - SamDocument1 pageCornelsen Einstufung Test (Abraham Brew - SamBrew-sam ABPas encore d'évaluation
- Nerve AnswersDocument9 pagesNerve AnswersBrew-sam ABPas encore d'évaluation
- Learning & Memory 2: NeuroethologyDocument53 pagesLearning & Memory 2: NeuroethologyBrew-sam ABPas encore d'évaluation
- 7 Step by Step FFXDocument15 pages7 Step by Step FFXBrew-sam ABPas encore d'évaluation
- JNNP 2012 303926Document5 pagesJNNP 2012 303926Brew-sam ABPas encore d'évaluation
- Script Intracellular 2017Document14 pagesScript Intracellular 2017Brew-sam ABPas encore d'évaluation
- Gold Kacha Flyer 2012Document2 pagesGold Kacha Flyer 2012gustavus1Pas encore d'évaluation
- Error Rateio NorunDocument725 pagesError Rateio Norunmatheus felipePas encore d'évaluation
- Cruise Control (3RZ-FE)Document6 pagesCruise Control (3RZ-FE)Esteban LefontPas encore d'évaluation
- Contoh Resume Lamaran KerjaDocument3 pagesContoh Resume Lamaran KerjaDyaa WidyaaPas encore d'évaluation
- Cessna 525 LimitationsDocument16 pagesCessna 525 LimitationsCesar BanchoffPas encore d'évaluation
- BER-E222 PMDocument8 pagesBER-E222 PMItalo MendozaPas encore d'évaluation
- SD Mock TestDocument35 pagesSD Mock TestSAPCertificationPas encore d'évaluation
- 3 - Pitot-Static Inst, System & ADC - OcrDocument110 pages3 - Pitot-Static Inst, System & ADC - OcrtmhoangvnaPas encore d'évaluation
- Getting Familiar With Microsoft Word 2007 For WindowsDocument3 pagesGetting Familiar With Microsoft Word 2007 For WindowsRaymel HernandezPas encore d'évaluation
- Jill K. Hatanaka: San Joaquin County Office of Education 2707 Transworld Drive Stockton, CA 95206 209-401-2406Document3 pagesJill K. Hatanaka: San Joaquin County Office of Education 2707 Transworld Drive Stockton, CA 95206 209-401-2406api-114772135Pas encore d'évaluation
- CV Kevin Ikhwan Muhammad Pt. Hasakona BinaciptaDocument6 pagesCV Kevin Ikhwan Muhammad Pt. Hasakona BinaciptaKevin MuhammadPas encore d'évaluation
- Ethics Thesis PaperDocument15 pagesEthics Thesis PaperEric LeggettPas encore d'évaluation
- True 63Document2 pagesTrue 63stefanygomezPas encore d'évaluation
- Workshop Manual Automatic Transmission 30 40leDocument2 pagesWorkshop Manual Automatic Transmission 30 40leDony TedyantoPas encore d'évaluation
- Silent Sound Technology Seminar ReportDocument42 pagesSilent Sound Technology Seminar ReportSrinivas B India79% (14)
- AZ-Edit User ManualDocument288 pagesAZ-Edit User Manualdjjd40Pas encore d'évaluation
- Fuel System: Fuel Tank / Fuel Cock 4-1 Fuel Pump 4 - 2 Carburetor 4 - 3Document10 pagesFuel System: Fuel Tank / Fuel Cock 4-1 Fuel Pump 4 - 2 Carburetor 4 - 3Fabrizio FloresPas encore d'évaluation
- Astm D522Document2 pagesAstm D522swapon kumar shillPas encore d'évaluation
- BRF90Document10 pagesBRF90Lukas Van VuurenPas encore d'évaluation
- TMB 60Document2 pagesTMB 60oac08Pas encore d'évaluation
- Checklist of E/OHS Activities For Asbestos Management: Name of Publication DateDocument20 pagesChecklist of E/OHS Activities For Asbestos Management: Name of Publication DateidahssPas encore d'évaluation
- NeuCardio E12Document2 pagesNeuCardio E12Daniel ParPas encore d'évaluation
- Ahmed Zaiba's CV SalehDocument6 pagesAhmed Zaiba's CV SalehSarah ZaibaPas encore d'évaluation
- Background of UNITAR International UniversityDocument3 pagesBackground of UNITAR International UniversityAin NadiaPas encore d'évaluation
- Arranging ObjectsDocument17 pagesArranging ObjectsWarda SyedPas encore d'évaluation
- How-To Guide: Transaction Launcher (SAP CRM 7.0) .0Document22 pagesHow-To Guide: Transaction Launcher (SAP CRM 7.0) .0Satish DhondalayPas encore d'évaluation
- ASTM D 3786 Bursting Strength, Diaphragm MethodDocument1 pageASTM D 3786 Bursting Strength, Diaphragm MethodAfzal Sarfaraz100% (1)
- EPSON WF-6090, WF-6530, WF-6590 Series Service Manual Page 121-140Document20 pagesEPSON WF-6090, WF-6530, WF-6590 Series Service Manual Page 121-140Ion IonutPas encore d'évaluation