Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Precision Nutrition. Nutrient TimingDocument21 pagesPrecision Nutrition. Nutrient TimingPaolo AltoéPas encore d'évaluation
- Intestinal ObstructionDocument21 pagesIntestinal ObstructionBheru LalPas encore d'évaluation
- Delta Robot KinematicsDocument11 pagesDelta Robot KinematicssekinPas encore d'évaluation
- The Utopia of The Zero-OptionDocument25 pagesThe Utopia of The Zero-Optiontamarapro50% (2)
- Homeostasis: Proudly Presents byDocument23 pagesHomeostasis: Proudly Presents byBheru LalPas encore d'évaluation
- CNA LPN Curriculum 11 March 2013Document72 pagesCNA LPN Curriculum 11 March 2013Bheru LalPas encore d'évaluation
- Policy Guidelines For Nursing Education in Pakista - 220418 - 132804Document3 pagesPolicy Guidelines For Nursing Education in Pakista - 220418 - 132804Bheru LalPas encore d'évaluation
- Nutritional Assessment of Children AdmittedDocument8 pagesNutritional Assessment of Children AdmittedBheru LalPas encore d'évaluation
- Nursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripDocument262 pagesNursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripBheru LalPas encore d'évaluation
- CH 8 Digestive System: StructuresDocument18 pagesCH 8 Digestive System: StructuresBheru LalPas encore d'évaluation
- Intestinal ObstructionDocument12 pagesIntestinal ObstructionBheru LalPas encore d'évaluation
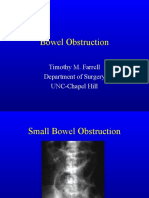
- Bowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillDocument27 pagesBowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillBheru LalPas encore d'évaluation
- Assessment and Management of Patients With Biliary DisordersDocument18 pagesAssessment and Management of Patients With Biliary DisordersBheru LalPas encore d'évaluation
- Intestinal Obstruction: Dr. Mohammad Jamil AlhashlamonDocument19 pagesIntestinal Obstruction: Dr. Mohammad Jamil AlhashlamonBheru LalPas encore d'évaluation
- WHO 2019 NCov IHR Ship Outbreak 2020Document12 pagesWHO 2019 NCov IHR Ship Outbreak 2020Bheru LalPas encore d'évaluation
- Science Since BabylonDocument224 pagesScience Since Babylonboris100% (1)
- The Challenge of Drug Discovery in The 21st CenturyDocument5 pagesThe Challenge of Drug Discovery in The 21st CenturyHugo de CeaPas encore d'évaluation
- Academic Calendar 2019-20 Odd Semester PDFDocument1 pageAcademic Calendar 2019-20 Odd Semester PDFPiyush ManwaniPas encore d'évaluation
- Transition Case StudyDocument4 pagesTransition Case StudyNobert BulindaPas encore d'évaluation
- Electoral Politics Module-2, Hand Out 2, Class 9, Civics, Lesson-3, Electoral PoliticsDocument4 pagesElectoral Politics Module-2, Hand Out 2, Class 9, Civics, Lesson-3, Electoral PoliticsSaiPas encore d'évaluation
- 2007 - Q1 NewsletterDocument20 pages2007 - Q1 NewsletterKisara YatiyawelaPas encore d'évaluation
- SMF Update Barang 05 Desember 2022Document58 pagesSMF Update Barang 05 Desember 2022Apotek Ibnu RusydPas encore d'évaluation
- SCHEEL, Bernd - Egyptian Metalworking and ToolsDocument36 pagesSCHEEL, Bernd - Egyptian Metalworking and ToolsSamara Dyva86% (7)
- Scottish Gaelic 2nd EditionDocument117 pagesScottish Gaelic 2nd EditionMila Akimova-LeePas encore d'évaluation
- NotesDocument2 pagesNotesNoella Marie BaronPas encore d'évaluation
- YCAP 7 Steps PosterDocument1 pageYCAP 7 Steps PosterSohila AmrPas encore d'évaluation
- Module 1 Lesson 1 Activity and Analysis: Special Needs EducationDocument2 pagesModule 1 Lesson 1 Activity and Analysis: Special Needs EducationShalyn ArimaoPas encore d'évaluation
- Making Effective Pres. Academic Lit I. Weeks 4 5Document27 pagesMaking Effective Pres. Academic Lit I. Weeks 4 5irfanaPas encore d'évaluation
- GBS210099-Nguyen Manh Quan - 1004B - As01Document33 pagesGBS210099-Nguyen Manh Quan - 1004B - As01quannmgbs210099Pas encore d'évaluation
- Past Simple (Regular/Irregular Verbs)Document8 pagesPast Simple (Regular/Irregular Verbs)Pavle PopovicPas encore d'évaluation
- Beed 3a-Group 2 ResearchDocument65 pagesBeed 3a-Group 2 ResearchRose GilaPas encore d'évaluation
- The Divine Liturgy Syro Malankara ChurchDocument4 pagesThe Divine Liturgy Syro Malankara ChurchGian Marco TallutoPas encore d'évaluation
- Lesson Plan Tower of LondonDocument5 pagesLesson Plan Tower of Londonmacrinabratu4458Pas encore d'évaluation
- Filters SlideDocument17 pagesFilters SlideEmmanuel OkoroPas encore d'évaluation
- People Vs VictorDocument4 pagesPeople Vs VictorEryl YuPas encore d'évaluation
- Back To Basics MRODocument5 pagesBack To Basics MROrstein666Pas encore d'évaluation
- Hayat e Imam Abu Hanifa by Sheikh Muhammad Abu ZohraDocument383 pagesHayat e Imam Abu Hanifa by Sheikh Muhammad Abu ZohraShahood AhmedPas encore d'évaluation
- Articol de CercetareDocument3 pagesArticol de CercetareLuiza Carmen PîrvulescuPas encore d'évaluation
- Thousand 6, One Thousand 7, One Thousand 8, One Thousand 9, One Thousand 10Document7 pagesThousand 6, One Thousand 7, One Thousand 8, One Thousand 9, One Thousand 10Nhazie NyzePas encore d'évaluation
- LM3886Document24 pagesLM3886moacirjmPas encore d'évaluation
- WWW Foboko Com Sentence Dictionary English UnderstandDocument12 pagesWWW Foboko Com Sentence Dictionary English UnderstandEnkhee WefweePas encore d'évaluation
- Selvanathan-7e 17Document92 pagesSelvanathan-7e 17Linh ChiPas encore d'évaluation