Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Intestinal ObstructionDocument21 pagesIntestinal ObstructionBheru LalPas encore d'évaluation
- Homeostasis: Proudly Presents byDocument23 pagesHomeostasis: Proudly Presents byBheru LalPas encore d'évaluation
- CNA LPN Curriculum 11 March 2013Document72 pagesCNA LPN Curriculum 11 March 2013Bheru LalPas encore d'évaluation
- Policy Guidelines For Nursing Education in Pakista - 220418 - 132804Document3 pagesPolicy Guidelines For Nursing Education in Pakista - 220418 - 132804Bheru LalPas encore d'évaluation
- Nursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripDocument262 pagesNursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripBheru LalPas encore d'évaluation
- Nutritional Assessment of Children AdmittedDocument8 pagesNutritional Assessment of Children AdmittedBheru LalPas encore d'évaluation
- Intestinal ObstructionDocument12 pagesIntestinal ObstructionBheru LalPas encore d'évaluation
- CH 8 Digestive System: StructuresDocument18 pagesCH 8 Digestive System: StructuresBheru LalPas encore d'évaluation
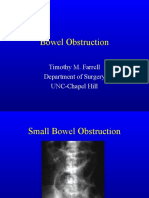
- Bowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillDocument27 pagesBowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillBheru LalPas encore d'évaluation
- Assessment and Management of Patients With Biliary DisordersDocument18 pagesAssessment and Management of Patients With Biliary DisordersBheru LalPas encore d'évaluation
- Intestinal Obstruction: Dr. Mohammad Jamil AlhashlamonDocument19 pagesIntestinal Obstruction: Dr. Mohammad Jamil AlhashlamonBheru LalPas encore d'évaluation
- WHO 2019 NCov IHR Ship Outbreak 2020Document12 pagesWHO 2019 NCov IHR Ship Outbreak 2020Bheru LalPas encore d'évaluation
- Language Dysfunction - Continnum - 2015Document19 pagesLanguage Dysfunction - Continnum - 2015Carolina Posada OrtizPas encore d'évaluation
- The Effect of Mindset On Decision-MakingDocument27 pagesThe Effect of Mindset On Decision-MakingJessica PhamPas encore d'évaluation
- Intro To Writing q2Document7 pagesIntro To Writing q2noreen diorPas encore d'évaluation
- What Is Pair ProgrammingDocument4 pagesWhat Is Pair ProgrammingMalik AmmarPas encore d'évaluation
- Are Old Parents Are Burden To Modern SocietyDocument2 pagesAre Old Parents Are Burden To Modern Societyviv100% (4)
- Your Best Chance For: International OffersDocument9 pagesYour Best Chance For: International Offersumesh kumarPas encore d'évaluation
- TN Board Class 11 Basic Electrical Engineering TextbookDocument256 pagesTN Board Class 11 Basic Electrical Engineering TextbookJio TrickzonePas encore d'évaluation
- Building Your Weekly SDR Calendar-Peer Review Assignment-Mohamed AbdelrahmanDocument3 pagesBuilding Your Weekly SDR Calendar-Peer Review Assignment-Mohamed AbdelrahmanrtwthcdjwtPas encore d'évaluation
- Emergence of OBDocument4 pagesEmergence of OBBhavya VermaPas encore d'évaluation
- Non-Academic Achievement Scholarships For Current Students 2019/20Document5 pagesNon-Academic Achievement Scholarships For Current Students 2019/20Ho Ming ChoPas encore d'évaluation
- Resume To School PMKDocument4 pagesResume To School PMKPravisk Pravi KPas encore d'évaluation
- Engineering Industrial Training Student Guide SpreadDocument11 pagesEngineering Industrial Training Student Guide SpreadAkaash TangPas encore d'évaluation
- D'man - Mech - CTS - NSQF-5 SyllabusDocument58 pagesD'man - Mech - CTS - NSQF-5 SyllabusNitin B maskePas encore d'évaluation
- Auburn Core CurriculumDocument1 pageAuburn Core CurriculumLuisPadillaPas encore d'évaluation
- Telecoms Mini MBA Jun-Sept 2011Document8 pagesTelecoms Mini MBA Jun-Sept 2011Mahmoud SalahPas encore d'évaluation
- 32.kushtia (Life Old)Document6 pages32.kushtia (Life Old)Habib AliPas encore d'évaluation
- Algebraic FractionsDocument11 pagesAlgebraic FractionsSafiya Shiraz ImamudeenPas encore d'évaluation
- Grade 12 Q1 A1Document2 pagesGrade 12 Q1 A1Ma. Catherine PaternoPas encore d'évaluation
- Factors Affecting Reading PerformanceDocument10 pagesFactors Affecting Reading PerformanceKeith VilardePas encore d'évaluation
- Hiring Recent University Graduates Into Internal Audit Positions: Insights From Practicing Internal AuditorsDocument14 pagesHiring Recent University Graduates Into Internal Audit Positions: Insights From Practicing Internal AuditorsBrigitta Dyah KarismaPas encore d'évaluation
- STS Report TopicDocument2 pagesSTS Report TopicJunel SildoPas encore d'évaluation
- Examination: Session: Course Title: Semester: Course Code: Max Marks: Date: 3/10/2020 Time: 12pm To 11:59amDocument2 pagesExamination: Session: Course Title: Semester: Course Code: Max Marks: Date: 3/10/2020 Time: 12pm To 11:59amsaqib aliPas encore d'évaluation
- Academic TextDocument2 pagesAcademic TextCatherine ProndosoPas encore d'évaluation
- Iit Delhi PHD Thesis PDFDocument8 pagesIit Delhi PHD Thesis PDFWebsiteThatWillWriteAPaperForYouSavannah100% (2)
- Introduction - The Role of Business Research (19.01.10)Document27 pagesIntroduction - The Role of Business Research (19.01.10)sehaj01Pas encore d'évaluation
- Human Resources Officer CVDocument2 pagesHuman Resources Officer CVsreeharivzm_74762363Pas encore d'évaluation
- Masouda New CVDocument4 pagesMasouda New CVmasoudalatifi65Pas encore d'évaluation
- Soal Midtest of English Lesson Class X SMK It AlDocument2 pagesSoal Midtest of English Lesson Class X SMK It AlIrzie Irvan Nubageur ElfaridziPas encore d'évaluation
- Verbs Worksheet 5th English Grammar NTSEDocument2 pagesVerbs Worksheet 5th English Grammar NTSESuvashreePradhanPas encore d'évaluation
- English Test Unit 1 3rd GradeDocument3 pagesEnglish Test Unit 1 3rd GradeJasmín GálvezPas encore d'évaluation