THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 95, No.
1, 2000
© 2000 by Am. Coll. of Gastroenterology ISSN 0002-9270/00/$20.00
Published by Elsevier Science Inc. PII S0002-9270(99)00768-6
Intestinal Pseudo-Obstruction
and Acute Pandysautonomia
Associated With Epstein-Barr Virus Infection
M. Besnard, M.D., C. Faure, M.D., G. Fromont-Hankard, M.D.,
H. Ansart-Pirenne, M.D., M. Peuchmaur, M.D., J. P. Cezard, M.D., and J. Navarro, M.D.
Departments of Pediatric Gastroenterology and Pathology and Immunology Unit, Hôpital Robert Debré,
Paris, France
ABSTRACT adrenergic systems, or can be selective for only one. Gut
We report the association of neurological and intestinal motility depends on the electrical and contractile property of
disorders with the reactivation of Epstein-Barr virus (EBV) the smooth muscle, with intrinsic control by the enteric
in a child. This previously healthy 13-yr-old boy presented nervous system and extrinsic control by the autonomic system.
with pharyngitis and acute abdominal ileus. Laparotomy Pandysautonomia could therefore lead to intestinal paresia.
excluded a mechanical obstruction. Postoperatively, he suf- One case of intestinal pseudo-obstruction due to autonomic
fered from prolonged intestinal obstruction, pandysautono- dysfunction in association with EBV infection (2) has been
mia, and encephalomyelitis. Histological examination of the reported, but no association between EBV infection and lesions
appendix and a rectal biopsy taken 3 months after the onset of the intrinsic nervous system has yet been described except in
showed an absence of ganglion cells (appendix) and hy- a retrospective study in one patient with chronic symptoms (3).
poganglionosis (rectum), with a mononucleate inflamma- This report describes the case of a young patient who presented
tory infiltrate in close contact with the myenteric neural with acute pandysautonomia, intestinal pseudo-obstruction
plexuses. EBV-PCR was positive in the blood and cerebro- syndrome, histopathological lesions of acquired hypoganglion-
spinal fluid, and in situ hybridization with the Epstein-Barr nosis, and inflammatory infiltration of the enteric nervous sys-
virus encoded RNA probe showed positive cells throughout tem, together with EBV reactivation.
the appendix wall including the myenteric area, in a mes-
enteric lymph node, and in the gastric biopsies. EBV spon-
taneous lymphocytic proliferation was noted in the blood. CASE REPORT
The serology for EBV showed previous infection but anti- A 13-yr-old boy, born on the island of La Réunion, from
early antigen antibodies were present. No immunodefi- unrelated parents, was referred to the gastroenterology unit
ciency was found. Neurological and GI recovery occurred
of our institution for subacute persistent intestinal obstruc-
after 6 months of parenteral nutrition and bethanechol. The
tion. He had no familial or personal medical history, and his
omnipresence of EBV associated with the neurointestinal
growth was developing on ⫹ 2.5 SD. In August 1996, he
symptoms suggest that the virus was the causal agent. This
suddenly presented with pharyngitis and with fever that was
is the first documented case of acquired hypoganglionnosis
refractory to antibiotics. Ten days later, he was admitted in
due to EBV reactivation. (Am J Gastroenterol 2000;95:
emergency for an acute abdominal syndrome, including
280 –284. © 2000 by Am. Coll. of Gastroenterology)
vomiting, abdominal pain, weight loss (2 kg), poor general
condition, and fever. His abdomen was tender and an ex-
ploratory laparotomy was performed; no visceral injury was
INTRODUCTION
found (the small bowel was not dilated), and the peritoneal
Epstein-Barr virus (EBV) can be responsible for a wide fluid was sterile. The appendix and a mesenteric lymph node
range of disorders including hepatitis, pancreatitis, and se- were resected. Postoperative outcome was marked by sub-
vere neurological impairments due to encephalomyelitis, or obstruction that needed prolonged gastric aspiration, paro-
polyneuropathies. However, there have been few reports of tiditis, pancreatitis (lipasemia 1200 U/L (normal ⬍ 40U/L)),
the autonomic nervous system involvement in association hepatitis (transaminases 300 U/L (normal ⬍ 45 U/L), or-
with infectious mononucleosis (1). Dysautonomia can be thostatic malaise, altered consciousness, and seizures. Sub-
associated with metabolic disorders (diabetes, amyloidosis, obstruction and a loss of 9 kg indicated prolonged total
etc.), viral infections, or toxic disease; or it can be idio- parenteral nutrition, for which he was transferred. A pyra-
pathic. Autonomic dysfunction can involve both the cholin- midal syndrome of the lower limbs and signs of encepha-
ergic (parasympathetic and sudoromotor sympathetic) and lomyelitis were also noted. Lumbar puncture showed nor-
AJG – January, 2000 Intestinal Pseudo-Obstruction, Dysautonomia, and EBV Infection 281
mal cerebrospinal fluid protein, cytology, and sterile culture.
Cerebral CT was unremarkable. Local infectious agents
were eliminated and his serology was ancient for EBV (IgG
VCA 1/160) and for cytomegalovirus.
When he was admitted to our unit, he still had signs of
pandysautonomia with a persistant fever (38.5°), vesical
retention, orthostatic hypotension, and unvariable pulse (60/
min). Clinical examination revealed intestinal subobstruc-
tion, bilateral pyramidal syndrome, and decreased muscular
strength and peripheral sensitivity to a pin prick on the feet.
His counsciousness was fluctuant. The right pupil was di-
lated and unreactive to light. He also had a sicca syndrome
with asialia, alacrymia, severe keratitis, and anhydrosis. A
second lumbar puncture was normal (cerebrospinal fluid
protein and lactic acid), as was the protein electrophoresis
pattern, but the EBV-PCR was positive. Cerebral MRI
showed a T2 hypersignal in the white matter. The electro-
encephalogram showed slow posterior waves and mild, non-
specific anomalies. The electromyogram was moderately
perturbed, with signs of peripheral neuropathy. Pandysau-
tonomia was documented with anhydrosis on the sweat
tests, abnormal ocular response to pilocarpine and atropine
showing abnormal parasympathetic reflex of the pupils,
abnormal heart rate recording and head-up tilting test to 30°
(systolic tension fell to 35 mm Hg). Polysomnography
showed no decrease of sensitivity of the respiratory center to
CO2 or defective ventilatory adaptation suggesting the ab-
sence of involvement of the respiratory center in the dys-
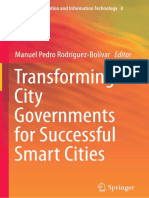
autonomia. The upper GI tests revealed a stenotic ileum
alternating with dilated loops and a normal jejunum (Fig. 1) Figure 1. Initial upper digestive tract opacification. Note the ste-
and diverticula all along the colon on the late x-rays. The notic ileum alternating with dilated loops with normal jejunum.
barium enema was normal. GI manometry was performed,
but the proximal jejunal record failed and esophageal record tive for HIV, HTLV1, hepatitis, and trypanosomiases, and
showed low amplitudes of the waves with abnormal prop- were ancient for cytomegalovirus, measles, rubella, and
agation of the distal two-thirds of the esophagus; rectal arboviruses. Immunological tests excluded classical immu-
manometry was normal. Urinary ultrasound examination nodeficiency and autoimmunity (absence of enteric neuronal
showed an initial megacystis with a sediment from poor autoantibody).
emptying and candidal urinary infection. A full-thickness Outcome
rectal biopsy specimen was taken 5 cm above the anal verge The patient was treated with polyvalent immunoglobulin
3 months after the onset of pandysautonomia. Biopsies were (0.5 g/kg/day for 5 days), but this treatment was ineffective.
also taken of the sural nerve, muscle, salivary gland, and Parenteral nutrition and bethanechol (0.5 mg/kg/day) al-
liver 6 months after the onset of the disease. lowed gradual GI remission and improvement of the neu-
rovegetative and counsciousness disturbances. Bladder
Laboratory Tests catheterization was necessary for 3 wk, after which the
Complete blood cell count was normal, but the erythrocyte patient began to void spontaneously. Gastric aspirate de-
sedimentation rate was elevated (100 mm at h 1). EBV creased and bowel movements appeared. Oral feeding re-
serologies showed ancient infection (positive IgG VCA placed parenteral nutrition 3 months after its beginning. The
1/160 and IgG EBNA 1/20). Four months after the onset, barium x-rays improved in April 1997. Only mild pupil
antiearly antigen antibodies were positive (1/80) and there dilation, occasional vomiting and constipation persisted. He
was a positive EBV-PCR both in serum (30 –300 copies/ was discharged and returned to the island of La Réunion in
1.5.105 mononucleated cells) and in the cerebrospinal fluid, May 1997, with a low-fiber diet and bethanechol. He re-
suggesting reactivation of the infection. Repeated blood mains well 12 months later.
tests showed persistent spontaneous proliferation of EBV
and a persistent inflammatory syndrome. Lactic acid was Pathology Methods
normal. Mitochondrial enzyme analysis on fresh-frozen The surgical specimens (appendix and mesenteric lymph
skeletal muscle was normal. Exhaustive checks were nega- node) were fixed in 10% formalin, embedded in paraffin, cut
282 Besnard et al. AJG – Vol. 95, No. 1, 2000
Figure 2. Muscular layers of the appendix: immunostaining with Figure 3. Staining with the EBER probe in the appendix evidences
anti-CD68 antibody shows numerous inflammatory cells com- EBER-positive cells in both the mucosa and the myenteric area
posed mainly of macrophages, grouped in clusters in the myenteric (insert) (⫻400, ⫻600).
area (X 250).
with a mild inflammatory infiltrate, containing mainly T-
5 m, and stained with hematoxylin and eosin. The biopsy cells, in the lamina propria and inside the nervous structures
specimens were fixed in 10% formalin, and fresh samples (Fig. 5). No EBER-positive cell was found.
from the same sites were frozen in liquid nitrogen. Immu- The gastric biopsies revealed lesions of nonatrophic
nohistochemical staining was performed on formalin-fixed chronic gastritis, with a diffuse mononuclear infiltrate in the
tissues using a streptavidin-biotin immunoperoxidase lamina propria. The inflammatory cells were mainly T-cells
method, with antibodies directed against: neuron-specific with a few plasma cells. HLA DR was overabundant on
enolase (NSE, Dakopatts, Glostrup, Denmark), T cells epithelial cells. EBER-positive cells were found scattered
(CD45RO, Dakopatts), and macrophages (CD68, Dako- within the infiltrate. No Helicobacter pylori was found.
patts). Immunohistochemistry was done on frozen tissue A biopsy of the sural nerve showed an axonal neuropathy
sections using an indirect immunoperoxidase technique with and a mild mononuclear cell infiltrate. The muscular biopsy
antibodies directed against: T cells (CD3, CD2, CD5, and excluded mitochondrial cytopathy and showed nonspecific
CD7, Becton Dickenson, Mountainview, CA), B cells (CD22, denervation. The salivary gland and liver biopsies showed
Dakopatts), macrophages (CD68, Dakopatts), and HLA DR nonspecific, mild inflammatory infiltrate of T cells, within
(Becton Dickenson). In situ hybridization was performed on the portal areas. No EBER- positive cells were noted.
formalin-fixed tissues with the Epstein-Barr virus encoded
RNA (EBER) probe (Dakopatts) according to the manufac-
turer’s recommendations. DISCUSSION
Results Our patient suffered from severe acute pandysautonomia
Histological examination of the appendix showed the ab- and intestinal pseudo-obstruction resulting from EBV reac-
sence of ganglion cells in both the submucosal and myen- tivation. The symptoms of autonomic dysfunction included
teric areas. This feature was associated with an inflamma-
tory infiltrate composed of mononuclear cells, mainly
located in the intestinal muscle. The inflammatory cells
were grouped in small clusters in the myenteric area (Fig. 2).
No acute appendicitis was found. Immunohistochemical
staining with NSE confirmed the absence of ganglion cells
from the appendix wall. The inflammatory infiltrate was
mainly of CD68-positive macrophages, and CD45RO-
positive T cells. Staining with the EBER probe showed
EBER-positive cells scattered throughout the appendix wall,
including the myenteric area (Fig. 3). Numerous EBER-
positive cells were also found within the mesenteric lymph
node.
The full thickness rectal biopsy revealed a markedly
reduced number of ganglion cells (maximum, 2 per section), Figure 4. Full-thickness rectal biopsy. Large hyperplastic nerve
with large hyperplastic nerve trunks in the submucosal and trunk in the myenteric area with rare ganglion cells (arrow) (he-
the myenteric areas (Fig. 4). These features were associated matoxylin and eosin, ⫻250).
AJG – January, 2000 Intestinal Pseudo-Obstruction, Dysautonomia, and EBV Infection 283
showed normal submucosal and myenteric ganglions with
no evidence of inflammation, so that the bowel dysmotility
was due to the dysfunction of the autonomic nervous sys-
tem, as in other reported cases of dysautonomia (4, 8, 14).
In the other case, there was evidence of chronic inflamma-
tory infiltrate involving the myenteric plexus with presence
of EBV in the Schwann cells demonstrated by in situ hy-
bridization (EBER probe). In our patient, the gut dysmotility
might have resulted from the abdominal vagal dysfunction
due to the dysautonomia, and from the destruction of the
enteric neurons by the postviral immune infiltrate. The in-
volvement of the enteric nervous system might result from
a direct viral injury or an abnormal T-cell immune response.
Figure 5. Full thickness rectal biopsy. Immunostaining with anti- Direct viral injury was reported in a case of intestinal
CD45RO antibody shows a mild mononuclear inflammatory infil- pseudo-obstruction related to cytomegalovirus infection
trate within the nerve trunks (⫻400). (15), with evidence of cytomegalovirus inclusions in the
enteric neurones. No EBER-positive enteric neuron was
found in our patient but, conversely, an immune-mediated
parasympathetic signs such as a lack of sweat, saliva, and
damage is supported by the presence of an inflammatory
tears; difficulties with micturition; pupil abnormalities; and
infiltrate, in close contact with the enteric plexuses, in both
sympathetic signs such as orthostatic hypotension, unvary-
the appendix, and the rectum.
ing pulse rate, and motor and sensory deficits. The first case
of acute acquired pandysautonomia was reported in 1969 by Acquired aganglionosis due to an immune process has
Young et al. (4); it particularly affected young people and been described, and it seems to be mainly of paraneoplastic
resulted in prolonged, incomplete recovery. Pandysautono- or autoimmune origin (16 –19). The main evidence for im-
mia has also been reported in cases of autoimmune disorders mune destruction of the enteric nervous system was the
(lupus), porphyria, botulism, posttraumatic, and hypotha- favorable response to steroid therapy. Our patient was given
lamic dysfunction (5–7). Only 20% of the reported cases of an immunomodulatory treatment with intravenous IgG in
pandysautonomia had been temporally associated with viral case it was an immunoallergic reaction (1, 20). No immu-
infections, such as EBV (8 –12). In the present case, all nosuppressor or antiinflammatory drug was given because
known causes of pandysautonomia were excluded, except of the spontaneous proliferation of EBV lymphocytes.
EBV infection. Our patient displayed signs of EBV reacti- The digestive symptoms associated with encephalomy-
vation, including circulating antiearly antigen antibodies, elitis may suggest a mitochondrial neurogastrointestinal en-
and a positive PCR-EBV in the serum and in the cerebro- cephalomyopathy (MNGIE) (21). In our patient, the clinical
spinal fluid. The ubiquitous presence of EBV was also presentation was atypical for such a diagnosis (absence of
indicated by spontaneous lineage, activated circulating T- ptosis, spontaneous clinical remission), metabolic investi-
cells, and EBER-positive cells in the mesenteric lymph node gations were negative (lactic acid in blood and in cerebro-
and appendix, and in the gastric biopsies. The temporal spinal fluid, absence of mitochondrial respiratory chain de-
association between the widespread presence of EBV and fect on fresh-frozen skeletal muscle analysis), and no lactic
signs of dysautonomia suggests that EBV was responsible acidosis episode occurred. The skeletal muscle biopsy was
for the neurological and GI disorders of our patient. The normal and the pathological findings were not suggestive of
most striking finding in the present case was the association MNGIE as no atrophy of the muscularis propria was noted.
of pandysautonomia with intestinal pseudo-obstruction. Gut The bilateral pyramidal syndrome was considered as related
dysfunction was most likely acquired, inamuch as the onset to the involvement of the central nervous system by the
was late in life, and because he has no past medical history EBV infection.
or growth failure. Gut dysfunction appeared quite acutely, In conclusion, this is, to our knowledge, the first docu-
probably aggravated by the surgery and the neurological mented case of acquired hypoganglionnosis related to EBV
impairment. GI x-rays excluded obstruction or structural reactivation. The spontaneous favorable outcome for both
disease, and manometry showed esophageal dysmotility, neurological and GI disorders might have depended on the
suggesting a neuropathic pseudo-obstruction. The colonic patient’s immunological ability to control virus reactivation.
diverticula were probably related to the motility distur-
bances of the GI tract, as noted in patients with intestinal
pseudoobstruction in POLIP syndrome (13). Reprint requests and correspondence: Christophe Faure, M.D.,
Only two cases of pseudo-obstruction associated with Service de Gastro-entérologie et nutrition pédiatriques, Hôpital
EBV infection have been reported (2, 3). In the first case, Robert Debré, 48, boulevard Sérurier, 75019 Paris, France.
histological examination of a resected colon specimen Received June 26, 1998; accepted Dec. 11, 1998.
284 Besnard et al. AJG – Vol. 95, No. 1, 2000
REFERENCES 12. Fujii N, Tabira T, Shibasaki H, et al. Acute autonomic and
sensory neuropathy associated with elevated Epstein-Barr vi-
1. Benneth JL, Mahalingam R, Wellish MC, et al. Epstein-Barr. rus antibody titre. J Neurol Neurosurg Psychiatry 1982;45:
Virus associated acute autonomic neuropathy. Ann Neurol 656 – 61.
1996;40:453–5. 13. Simon LT, Houroupian DS, Dorfman LJ, et al. Polyneurop-
2. Vassallo M, Camilleri M, Caron BL, et al. Gastrointestinal athy, opthalmoplegia, leukoencephalopathy, and intestinal
motor dysfunction in acquired selective cholinergic dysauto- pseudo-obstruction. POLIP syndrome. Ann Neurol 1990;28:
nomia associated with infectious mononucleosis. Gastroenter- 349 –360
ology 1991;100:252– 8. 14. Camilleri M, Malagelada JR, Stanghellini V, et al. Gastroin-
3. Debinski HS, Kamm MA, Talbot IC, et al.. DNA viruses in the testinal motility disturbances in patients with orthostatic hy-
pathogenesis of sporadic chronic idiopathic intestinal pseudo- potension. Gastroenterology 1985;88:1852–9.
obstruction. Gut 1997;41:100 – 6 15. Sonsino E, Mouy R, Foucaud P, et al. Intestinal pseudo-
4. Young RR, Asbury AK, Corbett JL, et al. Pure pandysauto- obstruction related to cytomegalovirus infection of myenteric
nomia with recovery. Brain 1975;98:613–36. plexus. N Engl J Med 1984;311:196 –7
5. Takayama H, Kazahaya Y, Kashihara N, et al.. A case of 16. Lennon VA, Sas DF, Busk MF, et al. Enteric neural autoan-
panganglionic cholinergic dysautonomia. J Neurol Neurosurg tibodies in pseudo-obstruction with small-cell lung carcinoma.
Psychiatry 1987;50:915– 8. Gastroenterology 1991;100:137– 42.
6. Edelman J, Gubbay SS, Zilko PJ. Acute pandysautonomia due 17. Gerl A, Storck M, Schalhorn A, et al. Paraneoplastic chronic
to mixed connective tissue disease. Aust New Zealand J Med intestinal pseudo-obstruction as a rare complication of bron-
1981;11:68 –70. chial carcinoid. Gut 1992;33:1000 –3.
7. Arruda WO, Teive HG, Ramina R, et al. Autonomic neurop- 18. Horoupian DS, Kim Y. Encephalomyeloneuropathy with gan-
athy in systemic lupus erythematous. J Neurol Neurosurg glionitis of the myenteric plexus in the absence of cancer. Ann
Psychiatry 1989;52:539 – 47. Neurol 1982;6:628 –32.
8. Yahr MD, Frontera AT. Acute autonomic neuropathy. Its 19. Smith VV, Gregson N, Foggensteiner L, et al. Acquired in-
occurrence in infectious mononucleosis. Arch Neurol 1975; testinal aganglionosis and circulating autoantibodies without
32:132–3. neoplasia or other neural involvement. Gastroenterology 1997;
9. Thomashefsky AJ, Horwitz SJ, Feingold MH. Acute auto- 112:1366 –71.
nomic neuropathy. Neurology 1972;22:251–5. 20. Heafield MTE, Gammage MD, Nightingale S, et al. Idiopathic
10. Low PA, Dyck PJ, Lambert EH, et al. Acute panautonomic dysautonomia treated with intravenous immunoglobulin. Lan-
neuropathy. Ann Neurol 1983;13:412–7. cet 1996;347:28 –9.
11. Neville BGR, Sladen GE. Acute autonomic neuropathy fol- 21. Perez-Atayde AR, Fox V, Teitelbaum JE, et al. Mitochondrial
lowing primary herpes simplex infection. J Neurol Neurosurg neurogastrointestinal encephalomyopathy: Diagnosis by rectal
Psychiatry 1984;47:648 –50. biopsy. Am J Surg Pathol 1998;22:1141–7.
Vous aimerez peut-être aussi
- The Quality of Care For MedicareDocument8 pagesThe Quality of Care For MedicareSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Hepatic Tissue Endothelin-1 PDFDocument5 pagesHepatic Tissue Endothelin-1 PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Twenty-Four-Hour Intragastric PH PDFDocument5 pagesTwenty-Four-Hour Intragastric PH PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- The Utility of CA 19-9 in The PDFDocument4 pagesThe Utility of CA 19-9 in The PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- The Long-Term Reinfection Rate and The Course PDFDocument7 pagesThe Long-Term Reinfection Rate and The Course PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Risk Factors For Irritable Bowel Syndrome PDFDocument9 pagesRisk Factors For Irritable Bowel Syndrome PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- The Striking Effect of HyperbaricDocument4 pagesThe Striking Effect of HyperbaricSyeda Ayesha Saleem HashmiPas encore d'évaluation
- The SIBDQ Further ValidationDocument7 pagesThe SIBDQ Further ValidationSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Role of ERCP in Asymptomatic Orthotopic Liver PDFDocument4 pagesRole of ERCP in Asymptomatic Orthotopic Liver PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Standardization of A Simplified PDFDocument9 pagesStandardization of A Simplified PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Tamoxifen-Induced Transient PDFDocument3 pagesTamoxifen-Induced Transient PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Isolated Abdominal Vasculitis PDFDocument2 pagesIsolated Abdominal Vasculitis PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Precipitation of Iron Overload and PDFDocument3 pagesPrecipitation of Iron Overload and PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Role of Hepatitis B Virus in PDFDocument9 pagesRole of Hepatitis B Virus in PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Rapid Onset of Massive PDFDocument2 pagesRapid Onset of Massive PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- H. Pylori in The Pathogenesis of PDFDocument5 pagesH. Pylori in The Pathogenesis of PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Risk of Fractures in Celiac Disease Patients PDFDocument7 pagesRisk of Fractures in Celiac Disease Patients PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Proximal Migration of Esophageal PDFDocument6 pagesProximal Migration of Esophageal PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Impact of Surgery For Crohn's PDFDocument6 pagesImpact of Surgery For Crohn's PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Pantoprazole Versus Ranitidine in The Treatment PDFDocument5 pagesPantoprazole Versus Ranitidine in The Treatment PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Metastatic Jejunal VIPoma PDFDocument5 pagesMetastatic Jejunal VIPoma PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Symptomatic Benefit 1-3 Years After PDFDocument5 pagesSymptomatic Benefit 1-3 Years After PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Long-Term Effects of Pyloromyotomy On PDFDocument9 pagesLong-Term Effects of Pyloromyotomy On PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Expression of Brain-Type PDFDocument9 pagesExpression of Brain-Type PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Increased Frequency of PDFDocument6 pagesIncreased Frequency of PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Clinical and Manometric Features PDFDocument7 pagesClinical and Manometric Features PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Hepatotoxicity Due To Troglitazone PDFDocument5 pagesHepatotoxicity Due To Troglitazone PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Comparative, Open, Randomized Trial PDFDocument5 pagesComparative, Open, Randomized Trial PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- Congenital Esophageal Stenosis in Adults PDFDocument5 pagesCongenital Esophageal Stenosis in Adults PDFSyeda Ayesha Saleem HashmiPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Lista 30 JulioDocument2 pagesLista 30 JulioMax Bike MartinezPas encore d'évaluation
- Simplex-4004 Installation Operating Manual Rev C PDFDocument36 pagesSimplex-4004 Installation Operating Manual Rev C PDFElias Rangel100% (1)
- Cost Accounting DQ - Midterms - AnswersDocument10 pagesCost Accounting DQ - Midterms - AnswersKurt dela TorrePas encore d'évaluation
- On Hereditary Italian WitchcraftDocument79 pagesOn Hereditary Italian WitchcraftAlbion JamesPas encore d'évaluation
- Department of Computer Applications Iii Semester Mc5304-Programming With JavaDocument32 pagesDepartment of Computer Applications Iii Semester Mc5304-Programming With JavaManibharathiPas encore d'évaluation
- Service ManualDocument14 pagesService ManualOlegPas encore d'évaluation
- Medical ParasitologyDocument33 pagesMedical ParasitologyAlexander Luie Jhames SaritaPas encore d'évaluation
- Drift Punch: Product Features ProfilesDocument3 pagesDrift Punch: Product Features ProfilesPutra KurniaPas encore d'évaluation
- Transforming City Governments For Successful Smart CitiesDocument194 pagesTransforming City Governments For Successful Smart CitiesTri Ramdani100% (2)
- The CardiacDocument7 pagesThe CardiacCake ManPas encore d'évaluation
- Mo Handbook Fbimnci Apr 18, 2019Document296 pagesMo Handbook Fbimnci Apr 18, 2019Prakash Thakulla100% (1)
- 2021.01 - Key-Findings - Green Bond Premium - ENDocument6 pages2021.01 - Key-Findings - Green Bond Premium - ENlypozPas encore d'évaluation
- Salting-Out Crystallisation Using NH Ina Laboratory-Scale Gas Lift ReactorDocument10 pagesSalting-Out Crystallisation Using NH Ina Laboratory-Scale Gas Lift ReactorChester LowreyPas encore d'évaluation
- PCM320 IDM320 NIM220 PMM310 Base Release Notes 1210Document48 pagesPCM320 IDM320 NIM220 PMM310 Base Release Notes 1210Eduardo Lecaros CabelloPas encore d'évaluation
- DIRECTORS1Document28 pagesDIRECTORS1Ekta ChaudharyPas encore d'évaluation
- Logistic RegressionDocument17 pagesLogistic RegressionLovedeep Chaudhary100% (1)
- The Muscle and Strength Training Pyramid v2.0 Training by Eric Helms-9Document31 pagesThe Muscle and Strength Training Pyramid v2.0 Training by Eric Helms-9Hamada MansourPas encore d'évaluation
- (Macmillan Studies in Marketing Management) Frank Jefkins BSC (Econ), BA (Hons), MCAM, FIPR, MInstM, MAIE, ABC (Auth.) - Public Relations For Marketing Management-Palgrave Macmillan UK (1983)Document193 pages(Macmillan Studies in Marketing Management) Frank Jefkins BSC (Econ), BA (Hons), MCAM, FIPR, MInstM, MAIE, ABC (Auth.) - Public Relations For Marketing Management-Palgrave Macmillan UK (1983)Subhasis DasPas encore d'évaluation
- SITXWHS001 Participate in Safe Work Practices - Training ManualDocument82 pagesSITXWHS001 Participate in Safe Work Practices - Training ManualIsuru AbhimanPas encore d'évaluation
- Next-Generation Widebody Conversion: in Service From 2017 ONWARDSDocument6 pagesNext-Generation Widebody Conversion: in Service From 2017 ONWARDSAgusPas encore d'évaluation
- Application Sheet: Series CW SeriesDocument2 pagesApplication Sheet: Series CW SerieskamalPas encore d'évaluation
- Angel FishDocument1 pageAngel FishWilla CrowellPas encore d'évaluation
- Currency Exchnage FormatDocument1 pageCurrency Exchnage FormatSarvjeet SinghPas encore d'évaluation
- Martina: Available Colors For This VersionDocument2 pagesMartina: Available Colors For This VersionUmeshPas encore d'évaluation
- Manual Cisco - DPC3925Document106 pagesManual Cisco - DPC3925HábnerTeixeiraCostaPas encore d'évaluation
- Grand Central Terminal Mep Handbook 180323Document84 pagesGrand Central Terminal Mep Handbook 180323Pete A100% (1)
- Daraz PKDocument4 pagesDaraz PKshavais100% (1)
- Syed Shujauddin 124661163Document3 pagesSyed Shujauddin 124661163shujauddin11Pas encore d'évaluation
- Cardboard Dream HouseDocument1 pageCardboard Dream Houseapi-630719553Pas encore d'évaluation
- Semi Detailed Lesson Format BEEd 1Document2 pagesSemi Detailed Lesson Format BEEd 1Kristine BuenaventuraPas encore d'évaluation